Introduction
A number of studies have demonstrated that ion channels encoded by the ether-à-go-go-related gene1 (ERG1) play a role in regulating the contractile activity of cardiac myocytes (reviewed by Vandenberg et al. [1]). Moreover, there is increasing evidence demonstrating a role for ERG1in regulating smooth muscle cell contractility. ERG1encodes the pore-forming α-subunit of the delayed rectifier voltage-gated potassium channel, Kv11.1. Herein we refer to the ERG gene and the cognate mRNA as ‘KCNH2’, and ‘KCNH2 mRNA’, respectively, to the channel protein as ERG and to the functional channel as Kv11.1. In addition to ERG, Kv11.1 channels contain regulatory β-subunits [2,3], such as the single transmembrane domain protein potassium voltage-gated channel subfamily E members 2, encoded by the gene KCNE2 (mRNA referred to as ‘KCNE2 mRNA’, and channel protein referred to as KCNE2).
Kv11.1 channels are activated following action potentials and function to repolarize the cell membrane by conducting potassium ions (K+) out of the cell, which constitutes the rapid component of the delayed rectifier current IKr [4,5]. Repolarization terminates the action potential and the associated contraction.
Kv11.1 channels have been shown in rat stomach and murine portal vein [6-8], as well as in opossum oesophagus [9]. In addition, selective Kv11.1 channel blockers have been shown to increase contractility in rat stomach [6], mouse portal vein [8], opossum oesophagus [9], mouse and guinea pig gall bladder [10], bovine epididymis [11] and human and equine jejunum [12,13].These smooth muscles all exhibit spontaneous contractile activity, which is also a property of uterine smooth muscle [14].
Kv11.1 channels were initially linked to myometrial contractility by Aaronson et al., who demonstrated that tetraethyl ammonium (TEA)- and 4-aminopyridine (4-AP)-sensitive voltage-dependent K+ (Kv) channels played a role in regulating action potential duration in rat myometrium [15].Greenwood et al. later examined mouse ERG (mERG) expression and function, and confirmed the presence of both the ERG1a and ERG1b splice variants, with ERG1a expression being more abundant than that of ERG1b [16]. They found that KCNH2 mRNA abundance did not change throughout gestation or with the onset of labor, however, mRNAs encoding auxiliary subunits, namely KCNE2, were significantly up-regulated approaching term [16].
More recently, our group reported that human ERG1 (hERG1) and KCNE2 were present in pregnant human myometrium during late gestation and labor [17]. We found that Kv11.1 activity supressed the amplitude and duration of contractions prior to labor, thereby supporting a role for Kv11.1 activity in helping to maintain uterine quiescence [17]. Previous reports have indicated that KCNE2 co-expression with hERG1 was not necessarily inhibitory of Kv11.1 activity [18], however, we found that the onset of labor was associated with the increased expression of KCNE2 and the decreased responsiveness of myocytes to the Kv11.1 inhibitor, dofetilide [17]. Together these findings support an inhibitory role for KCNE2 in the context of regulating hERG1 in the myometrium. The evidence also suggests that Kv11.1 activity contributes to the electrophysiological mechanisms that regulate uterine contractions and that inhibition of the α-subunit, ERG1, by the β-subunit, KCNE2, may facilitate labor [17]. Interestingly, the mechanism for reducing Kv11.1 activity to facilitate labor appears to be dysregulated in obese women. Maternal obesity is associated with increased rates of labor induction, dysfunctional labor requiring Caesarean section (CS) delivery, longer pregnancies, as well as postpartum haemorrhage [19-21]. We reported that high body mass index (BMI) was associated with increased levels of hERG1 and reduced levels of KCNE2 in the myometrium [17]. Furthermore, high BMI was associated with heightened Kv11.1 activity in vitro, suggesting that the delayed and protracted labor often observed in obese women is linked to elevated Kv11.1 activity in the myometrium [17].
Genes encoding the progesterone receptor (PGR) [22-24], estrogen receptor 1 (ESR1) [23,25], oxytocin receptor (OXTR) [24,26,27] and prostaglandin-endoperoxide synthase 2 (PTGS2) [24,28] have been identified as key genes involved human parturition. There is now extensive published literature linking the myometrial regulation of these genes, among others, to the maintenance of uterine quiescence and the transition to a contractile phenotype at labor [29-31]. Uncovering an association between expression of these key genes and genes encoding the Kv11.1 channel would ascertain the involvement of this channel in the increased contractility of the myometrium at term and as part of the myometrial transformation leading to labor.
The aim of this study therefore was to determine whether expression of KCNH2 and KCNE2 in term non-laboring human myometrium correlate with the expression of PGR, ESR1, OXTR and PTGS2. We report that in term pregnancy, KCNH2 and KCNE2 are expressed coordinatedly with these key parturition-associated genes, thus strengthening the link between uterine contractility and K+ channel abundance in myometrial cells. Furthermore, this study examined the relationship of myometrial KCNH2 and KCNE2 mRNA abundance with BMI, and explored the expression of both genes in myometrial biopsies from preterm deliveries.
Materials and Methods
Consumables and reagents
Superscript III First Strand Synthesis System, Ultrapure Glycogen, Ultra Pure Agarose and Trackit 100 BP DNA ladder were purchased from Invitrogen (Carlsbad, USA). TRizol Reagent and Turbo DNA-free 50 reactions were from Ambion (Austin, USA). Alien QRT-PCR Inhibitor Alert 400 Reactions were purchased from Integrated Sciences Pty (Sydney, Australia). PCR primers were purchased from Sigma (St Louis, USA). The 2 mL 2.8 mm CK28-R Ceramic Bead Kit for the Precellys homogenizer (Bertin Instruments, France) were purchased from Thermo Fischer Scientific (Melbourne, Australia). L-Glutamine, Sodium Pyruvate, Gentamicin, HEPES and Dulbecco’s Modified Eagle Medium (DMEM) were obtained from Gibco (Carlsbad, USA). SYBR Green 2x Master mix was from Applied Biosystems (Carlsbad, USA).
Myometrial Tissue acquisition
These studies were approved by the Hunter and New England Area Human Research Ethics Committee and the University of Newcastle Human Ethics Committee (02/06/12/3.13). All participants gave informed written consent. Human myometrial samples (5 × 5 × 10 mm) were obtained from the lower uterine segment during elective CS of singleton pregnancies. Preterm samples ranged from 31 - 34 weeks gestation while term samples were 38.2 - 39.6 weeks gestation. Patient BMI range was 18.3 - 38.0, and all patients were not-in-labor. The indications for elective not-in-labor term CS were previous CS, placenta praevia, fetal distress or breach presentation. The indications for elective not-in-labor preterm CS were placenta increta, pre-eclampsia and low levels of amniotic fluid. Following delivery of the placenta, 5 units of syntocinon were administrated directly into an intravenous line as part of standard care for the prevention of postpartum hemorrhage. Samples were therefore exposed to oxytocin for a brief period of time (3 min). All myometrial samples were placed on ice in a serum-free media containing DMEM with high glucose, 2 mM L-glutamine, 1 mM sodium pyruvate, 40 µg/mL gentamicin and 10 mM HEPES for the transfer to the laboratory. Myometrial tissues were then cleared of serosa, fibrous or damaged tissue and visible blood vessels before being dissected into smaller pieces and washed in serum-free media to remove excess blood. Approximately 100 mg of tissue was snap frozen in liquid nitrogen for subsequent analysis.
RNA extraction, Reverse transcription and Real-time quantitative PCR
RNA was extracted from 100 mg of tissue using TRizol Reagent (Ambion, USA) according to the manufacture’s protocol. Homogenization of tissue in TRizol Reagent was performed using a Precellys24 homogenizer (Bertin Instruments, France). Following extraction, RNA samples were purified using the TURBO DNA-free kit (Ambion, USA). An ND-1000 spectrophotometer (NanoDrop Technologies, Inc., USA) was used to measure RNA concentration (absorbance at 260 nm (A260) and 280 nm (A280)) and purity. RNA integrity was checked by agarose gel electrophoresis. Each RNA sample (0.5 µg of total RNA) was spiked with 0.5 x 107 copies of Alien RNA(Integrated Sciences Pty, Australia) and reverse-transcribed using the Super Script III First-Strand Synthesis System with random hexamer primers (Invitrogen, USA). The Alien RNA transcript is an in vitro transcribed RNA molecule that is non-homologous to any known nucleic acids and as such was used as a housekeeping gene for these studies [32-34]. Quantitative real-time PCR was performed using an ABI 7500 Sequence Detector (Applied Biosystem, USA). No-reverse transcription (no-RT) negative controls were prepared for each sample to ensure there was no DNA contamination. The final volume of each PCR reaction was 20 µL containing 10 µL of 2x SYBR Green PCR Master Mix (Applied Biosystems, USA), master mix cDNA template (corresponding to 10 ng of reverse transcribed RNA), target cDNA-specific forward and reverse primers, and MilliQ water. For the reference gene (Alien primer), the final volume was also 20 µL with 1.0 µL of 2.5 µM of Alien Primer Mix, 10 µL of 2x SYBR Green PCR and the same amount of cDNA as the target genes and MilliQ water. No-template control samples (NTCs) were included in each PCR plate to detect any contamination and primer-dimers. PCR primers were designed using Primer Express, optimized and validated by confirming that single amplicons of appropriate size and sequence were generated (Table 1).
Data and statistical analysis
All mRNA abundance data were expressed relative to the Alien reference RNA. The relative mRNA abundance was calculated using the delta Ct (∆Ct) method [35]. All mRNA relative abundance values were then logarithmically transformed to approach normal distribution. Statistical analyses were conducted with Graph Pad Prism software (San Diego, CA, USA). Graphical data are presented as mean ± SEM. For comparison between two groups, Student’s t-test was used. For correlation studies Pearson’s product moment correlation coefficient was used (Pearson’s r). Preterm and term samples were compared by 1-way ANOVA with Bonferroni’s multiple comparisons test. P-values ≤ 0.05 were considered statistically significant.
Results
KCNH2and KCNE2 expression in human myometrium at term pregnancy
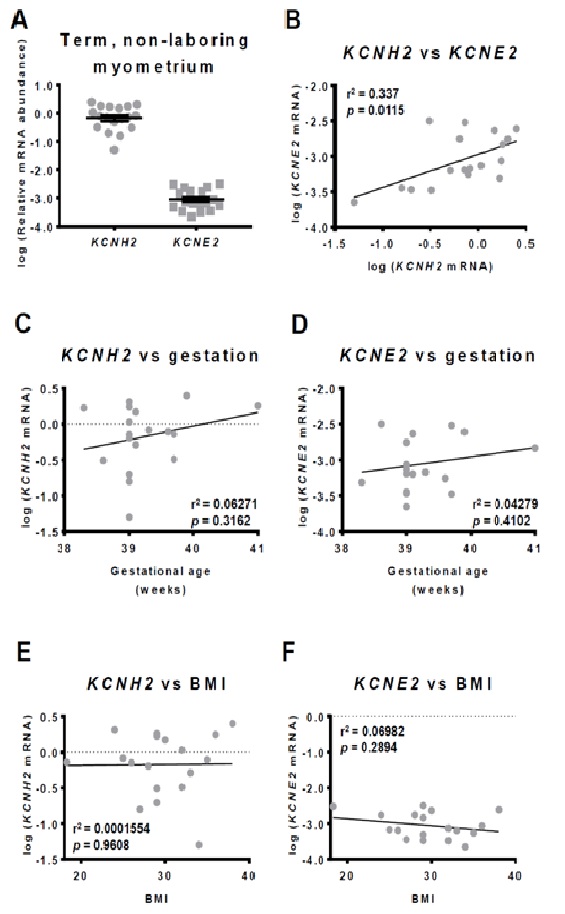
Relative abundance of KCNH2 and KCNE2 mRNA was measured in non-laboring term myometrial tissues (n=18). Expression of KCNH2 was much higher than of KCNE2 (over two orders of magnitude, Figure 1A). A statistically significant positive correlation was found between KCNH2 and KCNE2 mRNA abundance (r2=0.34, p=0.01) (Figure 1B).
There was no statistically significant relationship between KCNH2 mRNA abundance and gestational age (r2=0.06, p=0.31) (Figure 1C), or KCNE2 mRNA abundance and gestational age (r2=0.04, p=0.41) (Figure 1D) within the term gestation range of 38.2-41.0 weeks.
Since we have found previously that hERG1levels increase whilst KCNE2 levels decrease with increasing BMI of term pregnant women, we have correlated KCNH2 mRNA as well as KCNE2 mRNA abundance to BMI. The BMI in our patients group ranged from 18.3 to 38.0. There was no statistically significant correlation between KCNH2 mRNA abundance (r2=0.0002, p=0.96) (Figure 1E) or KCNE2 mRNA abundance and BMI (r2=0.07, p=0.29) (Figure 1F).
Correlations between the expression of KCNH2, KCNE2 and contraction-associated myometrial genes
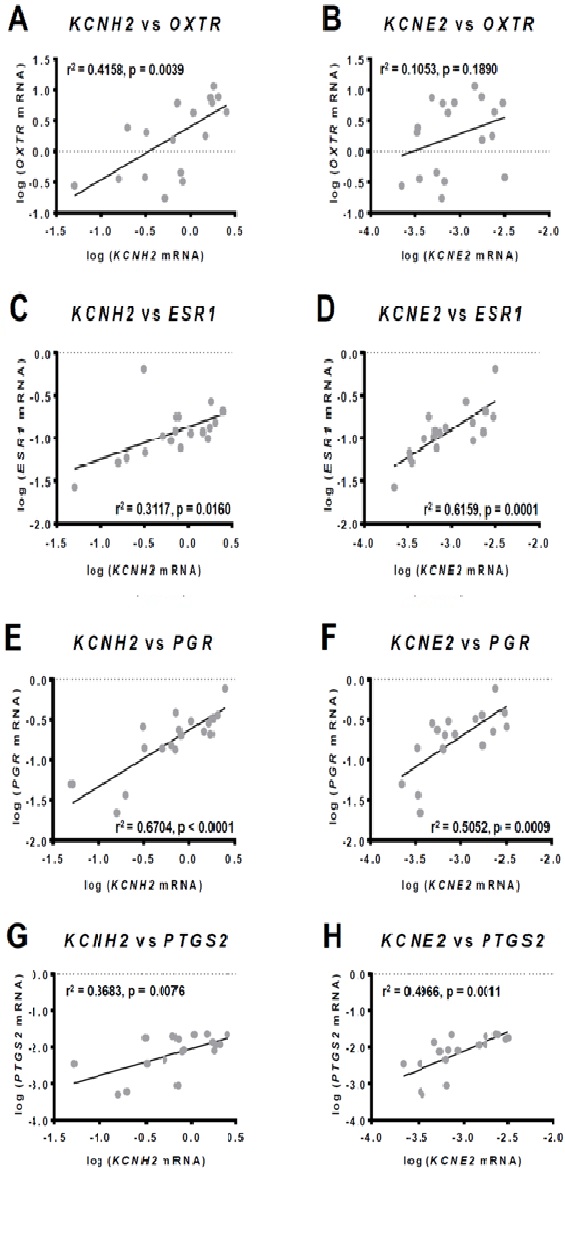
We measured the relative abundance of OXTR, ESR1, PGR and PTGS2 mRNAs (n=18 each) and correlated their abundance with KCNH2 and KCNE2 mRNA abundance. A statistically significant positive correlation was found between KCNH2 and OXTR (r2=0.42, p=0.0039) (Figure 2A) but not between KCNE2 and OXTR mRNA abundance (r2=0.11, p=0.19) (Figure 2B). ESR1 mRNA abundance was positively correlated with KCNH2 (r2=0.3117, p=0.0160) (Figure 2C) and KCNE2 mRNA abundance (r2=0.62, p=0.0001) (Figure 2D). Moreover, PGR mRNA also correlated positively with KCNH2 (r2=0.67, p<0.0001) (Figure 2E) and KCNE2 mRNA abundance(r2=0.51, p=0.0009) (Figure 2F). In our term non-laboring samples progesterone receptor A (PR-A) expression was barely detectable, meaning correlations with PGR were predominantly in relation to progesterone receptor B (PR-B). Finally, the key contraction-associated gene product, PTGS2 mRNA, also exhibited significant positive correlation with KCNH2 (r2=0.37, p=0.0076) (Figure 2G) and KCNE2 mRNA abundance (r2=0.50, p=0.0011) (Figure 2H).
KCNH2 and KCNE2 expression in preterm human myometrium
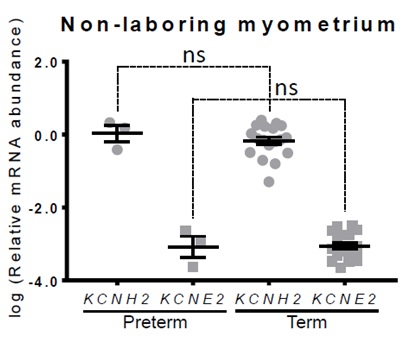
The relative abundance of KCNH2 and KCNE2 mRNA was determined in a limited number of non-laboring preterm myometrial tissues (n=3). No difference was found for KCNH2 (p=0.47) or KCNE2 (p=0.92) mRNA abundance compared to term non-laboring samples (n=18) (Figure 3).
Discussion
We previously reported the presence of hERG1 and KCNE2 in pregnant human myometrium in late gestation, and demonstrated that labor onset is associated with diminished Kv11.1 activity in association with enhanced expression of the inhibitory subunit, KCNE2 [17]. Furthermore, we reported a significant positive correlation between Kv11.1 activity and BMI, which was attributable to increased hERG1 levels and decreased KCNE2 levels [17].In follow up to that functional study, we examined KCNH2 and KCNE2 gene expression in term non-laboring myometrium and found that KCNE2 expression was relatively low, and correlated with KCNH2 expression. Moreover, the levels of both mRNAs correlated positively with the expression of myometrial genes that are key regulators of parturition, but showed no relationship with the BMI of the participants. Patients comprising our term non-laboring cohort ranged from underweight (BMI 18.3) to Class II obese (BMI 38.0) (World Health Organisation guidelines). The lack of correlation suggests that within the examined BMI range, the effect of obesity is not on KCNH2 or KCNE2 gene expression, but rather on protein levels. This finding refines the link between Kv11.1 activity and BMI, and suggests that future studies should focus on the effect of obesity on KCNH2 and KCNE2 mRNA translation as well as protein turnover.
Another potassium channel that plays a crucial role in pregnancy is the ATP-sensitive K+ (KATP) channel. KATP-mediated K+ efflux plays a role in maintaining the resting membrane potential of myocytes [36]. Several studies have found that in late pregnancy, the number of myometrial KATP channelsis reduced, which increases uterine excitability, thereby promoting the establishment of labor [37-39]. Du et al. [40] found that all KATP channel subunits, apart from the SUr2A subunit, were down-regulated in the late pregnant uterus compared to the non-pregnant uterus. More importantly, expression of SUr2B/Kir6.1 in term pregnant human myometrium was found to be increased in women older than 35 years [40]. Advanced maternal age is associated with increased obstetric risks in general, as well as increased risk of elective and emergency CS [41,42]. The study therefore suggests that increased risk of birth complications in women aged over 35 years may be linked to reduced myocyte excitability attributable to increased numbers of KATP channels in the myometrium [40]. This is consistent with our previous study on hERG1, which similarly links poor labor outcomes for obese women with the elevated activity of a potassium channel [17]. Both studies illustrate the importance of understanding how different potassium channels regulate uterine contractility, as dysregulation can lead to obstetric complications.
In pregnant human myometrium, we observed a significant positive correlation between KCNH2 and KCNE2 mRNA abundance at term (Figure 1B). This correlation, if it translates to protein abundance, could suggest an underlying subunit stoichiometry in myometrial Kv11.1 channels. Given that all term samples analysed were non-laboring, preservation of the high KCNH2:KCNE2 ratio may play a role in maintaining quiescence in non-laboring tissue.
The uterine quiescence, which persists for the majority of pregnancy, is maintained by inhibitors of uterine contraction, such as progesterone [24,43-46]. As term approaches there is a shift from progesterone to estrogen dominance and the uterus undergoes a phenotypic transition. This transition is characterised by up-regulated expression of a series of contraction-associated genes (reviewed by Smith [47]), including receptors for oxytocin and prostaglandins, increased expression of genes encoding myometrial gap junctions, such as connexin 43, which facilitates synchronous contractions, and alterations in resting membrane potential of myocytes, which renders myocytes more prone to excitation [24,43-46,48]. Collectively these changes increase the likelihood that sporadic contractions of the uterus will propagate in synchrony and lead to established labor [49]. In fulfilling a role as a regulator of myometrial contractility, it would therefore be reasonable to expect Kv11.1 activity, and thus KCNH2 and KCNE2 expression, to correlate with the expression of key genes that are known to play a role in this phenotypic transition.
OXTR expression in the myometrium is reportedly constant between 24 - 36 weeks gestation, but rises significantly in term samples (>37 weeks) prior to the onset of labor [48,50]. Within this latter time frame (term), we found that KCNH2 expression correlated positively with OXTR expression, whereas KCNE2 did not. Given that KCNH2 mRNA abundance is significantly correlated with both KCNE2 and OXTR mRNA abundance, a correlation should be expected between KCNE2 and OXTR mRNA levels. It is possible that with greater sample numbers a positive correlation would be demonstrated between KCNE2 and OXTR expression. Given that the role of Kv11.1 within the myometrium is to rapidly terminate contractions in order to prevent propagation of uterine contractility and the establishment of labor, it is reasonable to conjecture that KCNH2 expression is co-regulated with OXTR expression as a counter-measure to offset increased sensitivity to oxytocin.
Similar considerations may apply to the observed positive correlation of KCNH2 and KCNE2 with ESR1 and PTGS2. ESR1 encodes estrogen receptor α (ERα), which drives the estrogen-dependent expression of contraction-associated proteins, such as connexin 43 [51-54]. PTGS2 is responsible for the biosynthesis of prostaglandins (PGs). Prostaglandin F2α(PGF2α) is produced mainly by the maternal decidua and is involved in the up-regulation of OXTR levels and gap junctions in the myometrium, thus promoting uterine contractions [55]. Prostaglandin E2(PGE2) is produced by the fetus and placenta and is involved in collagen degradation and dilation of small blood vessels in the cervix, thus promoting cervical ripening as well as spontaneous rupture of the fetal membranes [56]. It is important to remain mindful, however, that non-laboring tissues were analysed in our study suggesting the possibility that women with high expression of ESR1 and PTGS2 may require higher levels of KCNH2 in order to maintain uterine quiescence than women with lower ESR1 and PTGS2 expression. Moreover, in the heart KCNE2 expression is up-regulated by estrogen [57]. Taking into consideration that in humans circulating levels of estrogen are high for most of pregnancy, and remain elevated during parturition [46,58], it is likely that estrogen regulation of KCNE2 expression, and thus Kv11.1 activity, plays an important role in modulating the transition from quiescence to contractility.
KCNH2 and KCNE2 mRNA levels were both positively correlated with PGR expression. Consistent with previous studies we report PGR total expression [30] as within our term non-laboring cohort PR-A expression was barely detectable. The strong positive correlations between KCNH2 and KCNE2 expression with PGR expression are therefore in relation to PR-B, which is consistent with the observed KCNH2:KCNE2 ratio potentially contributing to pregnancy maintenance. A follow up analyses determining whether KCNH2 and KCNE2 expression continue to correlate with PGR expression in laboring tissue would provide valuable insight into whether progesterone regulates hERG1 and KCNE2 levels as means of maintaining uterine quiescence.
In mice, KCNH2 expression remains constant across gestation and there is no change in ERG1 protein levels [16]. KCNE2, however, is gestationally regulated in mice in that mRNA abundance is significantly up-regulated by day 14 of a 20 day pregnancy, and KCNE2 protein levels are significantly up-regulated by day 17 [16]. Our analyses of preterm non-laboring samples showed no change in KCNH2 or KCNE2 gene expression earlier in gestation suggesting that, unlike mice, KCNE2 gene expression may not be gestationally regulated in humans. If confirmed by analysis of additional preterm samples, this could indicate that alternative auxiliary subunits need to be explored in the context of human myometrium. To date, studies exploring the role of Kv11.1 channels in human myometrium have focused on KCNE2 co-expression alongsidehERG1. However, a variety of auxiliary subunits are known to modulate Kv11.1 activity [1], and studies by Greenwood et al. [16] indicate that KCNE4 expression is gestationally regulated in mouse uterine tissue in addition to KCNE2. As such it is possible that KCNE4, or another regulatory subunit, is gestationally regulated in humans.
Conclusion
We have previously provided functional data examining the role of Kv11.1 in regulating myometrial contractility at term labor. Here we have followed up the functional study with an analysis of KCNH2 and KCNE2 gene expression in term non-laboring women. We have shown that KCNH2 and KCNE2 expression correlate with the expression of key myometrial genes implicated in parturition. Our data suggest that KCNH2 and KCNE2 are participants in the gene network controlling myometrial contractility at term. Uncovering this association advances our understanding of the mechanisms that underpin myometrial transformation, and reiterates the complexity of the parturition process. A complementary analysis using laboring myometrium would assist with the further interpretation of these results as alterations of the correlative network with the onset of labor would provide insight into which relationships are critical in maintaining uterine quiescence. We have also performed an initial investigation into KCNH2 and KCNE2 expression in preterm samples, which did not show any robust association between the preterm status and KCNH2 or KCNE2 expression. This investigation should be followed up with additional preterm samples to strengthen the study, as well as the analysis of preterm in-labor samples. Furthermore, future studies include examining whether these correlations translate into correlations at the protein level.
Acknowledgement
The authors wish to thank the obstetricians from the John Hunter Hospital, NSW, our research midwife, Anne Wright, and the research participants who donated samples toward this study.
Conflict of Interests Disclosure
Roger Smith holds a patent through the University of Newcastle in relation to the hERG potassium channel, titled “Compositions and methods for modulating uterine contractions”. The remaining authors declare that there is no conflict of interest regarding the publication of this paper.