Establishing Objectivity in the McCollough Facial Rejuvenation System
*Corresponding Author(s):
Gaylon McCollough EDepartment Of Facial Plastic And Reconstructive Surgery, McCollough Plastic Surgery Clinic, Cypress Bend Drive, Gulf Shores, Alabama, United States
Tel:+1 2519677600,
Fax:+1 2519677689
Email:drmccollough@mccolloughinstitute.com
Abstract
Importance
To bring focus on condition-specific treatment plans and improve comparability of various facial rejuvenation techniques and outcomes.
Objective
Provide objective criteria with which to validate the McCollough Facial Rejuvenation System.
Design
A prospective survey.
Setting
Private practice clinic.
Participants
Patients undergoing primary rhytidectomy between January 1, 2013 and December 31, 2013.
Main outcome measures
Intrarater and interrater reliability of the McCollough Facial Rejuvenation subscales, overall score, and stage of aging.
Results
The average intrarater Pearson correlation coefficient for the forehead is 0.77 (range 0.70-0.83), jowls is 0.77 (range 0.64-0.87), melolabial folds/marionette lines is 0.63 (range 0.44-0.80) and neck is 0.80 (range 0.54-0.90). The average intrarater Pearson correlation coefficient for the stages was 0.69 (range 0.63-0.80). The average interrater Pearson correlation coefficient for the stages at time 1 is 0.71 (range 0.60-0.84) and at time 2 is 0.62 (range 0.48-0.73).
Conclusions and relevance
The McCollough Facial Rejuvenation System, updated with objective criteria using previously validated subscales, has proven to have excellent INTRA and INTER rater reliability among a varied background of evaluators indicating its broad applicability.
Level of evidence
N/A.
Keywords
INTRODUCTION
| Stage | Total Points | Biological Age | Treatment Plans | |||
| I | 0-1 | The less-than-30 face-lift | For the younger individual who has little or no loose skin and may require only liposuction to remove unwanted fat and bulges | |||
| II | 2-4 | The 30-something face-lift | For the patient who is beginning to notice sagging of the brows and cheeks, but not the neck. Whenever sagging tissues are present, facial muscles and fat must be repositioned into their more youthful relationships. In such cases, a small amount of loose skin is removed. | |||
| III | 5-8 | The 40-something face-lift | For the patient who exhibits sagging brows, cheeks, and neck. Some of these patients may or may not need liposuction for contouring jowls and fullness under the chin. All, however, require suspension techniques to muscles and fat. | |||
| IV | 9-12 | The 50-something face-lift | For the patient with generalized facial and neck sagging, with or without jowls and wrinkles around the mouth. With more obvious muscle, fat, and skin laxity, more suspension of these structures is required. | |||
| V | 13+ | The 60-plus face-lift | For the patient with advanced aging, coupled with sagging of all facial areas including the forehead, brows, cheeks, and neck. At this stage in the aging process, deep folds develop in the groove between the nose and face, jowls droop below the jawline, and the muscle of the neck often produce string like bands that run vertically from the chin to the upper chest. Many of these patients are also beginning to exhibit wrinkles and blemishes over most of the face. | |||
This algorithm was further expanded in 2012 to provide a more user-friendly classification guide better defining the “language of surgical rejuvenation”. It provided appropriate descriptions of characteristics related to face-lifting, volume augmentation, and eyelid rejuvenation and added new descriptors to include the lips and earlobes to be more comprehensive. The purpose of the updated system was to further assist surgeons in developing a surgical plan for the separate regions based on the stage of aging, as opposed to a cookie cutter or one size fits all approach to facial rejuvenation [2]. Whereas objectivity is the goal of creating this facial rejuvenation staging system, this paper was still limited by the subjectivity of the classification system.
The goal of creating a facial classification system is not isolated to facial plastic surgery, but the goal of creating a condition-specific treatment plan to achieve total facial rejuvenation is. Other systems have been designed as scales to measure the aging face and the response to non-invasive cosmetic procedures such as filler injections and neuromodulators. Five-point photo numeric scales to assess brow position [3,4], forehead wrinkles [3,4], melolabial folds [3,5], marionette lines [3,5], jowls [5], and neck [6] have been developed and validated. Although not necessarily designed for preoperative surgical evaluation, these validated scales assess many of the same components as the McCollough Facial Rejuvenation System.
The purpose of this study is to introduce more objective, validated criteria to incorporate into the McCollough Facial Rejuvenation System to further improve its utility and applicability among aesthetic surgeons.
METHODS AND MATERIALS
For each patient, a total of 6 views were used for purposes of facial assessment (with the exception of one patient who lacked a left oblique view). These included frontal, bilateral obliques, bilateral profile, and a zoomed in view of the forehead/brow complex. A number was then placed on each photo sheet for purposes of record tracking but no personal information was included.
Although the McCollough Facial Rejuvenation System includes multiple subsites, sidedness, facial analysis, eye analysis, and skin texture, in order to begin the process of validation it was determined that focusing on one area at a time would provide the most utility and have the least variability. Therefore, the focus was on the facial analysis. The subunits of the face to be evaluated included the forehead, jowls, melolabial fold/marionette lines, and neck as they most correlated to the McCollough Facial Rejuvenation System forehead/temple (forehead), cheek (jowls and melolabial fold/marionette line), and neck.
Using the descriptions previously noted in the McCollough Facial Rejuvenation System and a series of photo numerical scales rated from 0-4 that had been previously validated [4-7], points were assigned to each stage (Table 1). For example, the patient who falls into a stage I would only have slight adiposity, usually seen in the jowl and submandibular regions. This would correlate to a forehead 0, melolabial fold/marionette line 0, jowls 1, and neck 0. Stage II patients have sagging of the brows and cheeks but not the neck. This correlates to a FH 0-1, melolabial folds/marionette lines 1, jowls 1-2, and neck 0 for a total of 2-4 points. Stage III patients are the 40 something patients. They exhibit sagging brows, cheeks, and necks. This would correlate to a FH 1-2, melolabial folds/marionette lines 1-2, jowls 1-2, and neck 1-2. The stage IV patient is the 50 something patient with generalized facial and neck sagging. This correlates to a FH 2-3, melolabial folds/marionette lines 3-4, jowls 1-3, and neck 3. The stage V patient is described having advanced aging, coupled with significant volume redistribution and sagging of all facial areas including the forehead, brows, cheeks, and neck. At this stage in the aging process, malar fat pads descend, hollowing occurs in the mid-cheek regions, deep folds develop in the groove between the nose and face (melolabial fold/marionette lines 4), jowls droop below the jawline (jowls 4), and the muscles of the neck often produce string like bands that run vertically from the chin to the upper chest (neck 3+). For the sagging of the forehead and brow this has the greatest variability in aging and was given the score of 2+ creating a total score of 13+ for stage V. A condition-specific treatment plan for each subsite was determined by the score assigned to that particular region. For example, an N-1 neck might only require liposuction, whereas an N-4 neck might require liposuction and platysmaplasty/myectomy with extensive SMAS suspension as seen in the patient in figure 1.
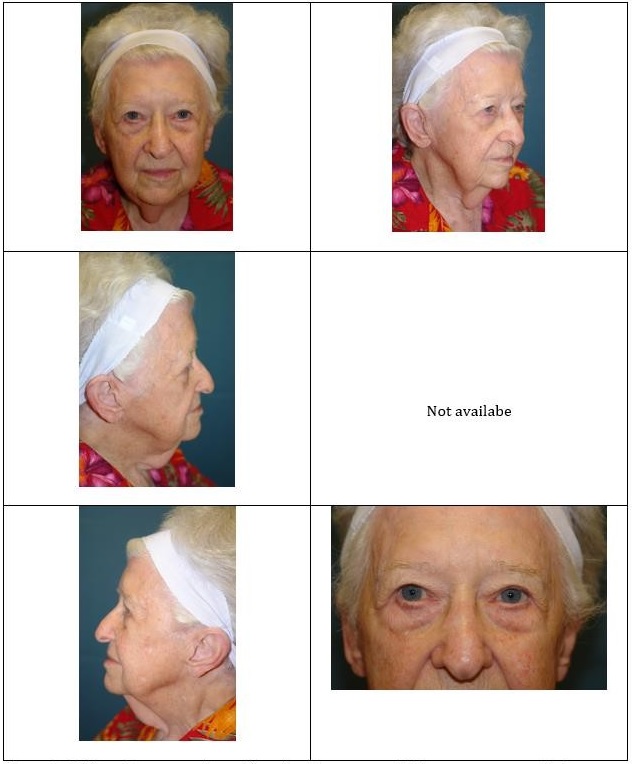
Figure 1: This patient was universally selected as a stage V. Her average score for forehead is 3.5 (range 3-4), fowls is 4 (range 4-4), melolabial fold/marionette lines is 4 (range 4-4), neck is 4 (range 4-4), and overall score is 15.5 (15-16).
The photonumeric scales coupled with written descriptions were then assembled as seen in table 2 and figure 2 which represents a computer generated morphing of the same patient with advancing degrees of aging. In cases where more than one criteria was assessed as in the forehead (brow position and wrinkles), points were assigned based on the more severely aged component (i.e., if they were wrinkle 2 and brow position 3 they were given a score of 3). The photo sheets for each patient were then evaluated by each of the four facial plastic surgeons (three board certified and fellowship trained and one currently in fellowship) and given a numerical score (0-4). An overall aging stage was calculated by adding the total numerical score based on table 1. This McCollough Facial Rejuvenation Stage was generated automatically by the addition of the points for each subsite.
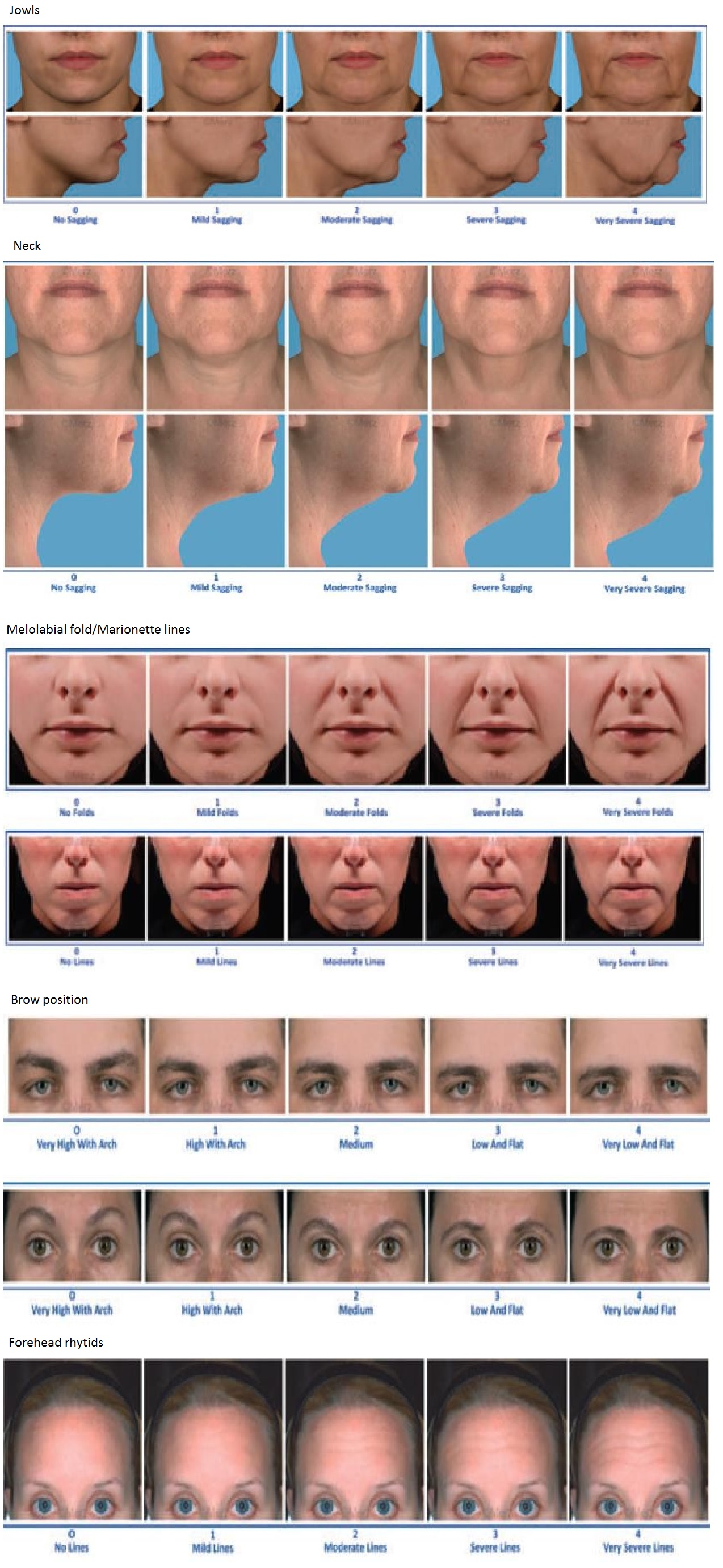
Figure 2: Visual scales for each facial sub site.
Note: Visual scales for facial analysis corresponding to the descriptions are provided in table 2.
| Points | |||||
| Region | 0 | 1 | 2 | 3 | 4 |
| Forehead | No wrinkles, very high brow with arch | Mild wrinkles, high brow with arch | Moderate wrinkles, medium brow position | Severe wrinkles, low and flat brow | Very Severe wrinkles, very low and flat brow |
| Melolabial fold/ Marionette Line | No visible folds, continuous skin line | Shallow but visible folds with slight indentation | Moderately deep folds, clear feature at normal appearance but not when stretched | Very long and deep folds; prominent facial feature | Extremely long and deep folds; detrimental facial appearance |
| Jowls | No jowling or superfluous adipose tissue | Mild jowling or superfluous adipose tissue. Lack of smooth jawline showing early signs of jowl formation | Moderate jowling or superfluous adipose tissue. Fullness in the lower cheek with visible marionette or melolabial fold | Severe jowling or superfluous adipose tissue. Greater fullness/heaviness of the lower cheek. Prominent melolabial fold. | Very severe jowling or superfluous adipose tissue. Greater prominence of the melolabial folds. Jowls below the level of the chin |
| Neck | No sagging, no loose skin | Mild sagging or mild loose skin | Moderate sagging or moderate loose skin | Severe sagging or moderate loose skin | Very severe sagging or severe loose skin |
The scores were recorded on a single sheet and provided to the primary author. After 30 days, the sheet with patient color photos was again sent to each evaluator for reevaluation of the faces. No attempt was made to randomize the order of the patients for the second facial analysis.
Using data points for the first and second evaluation time, a Pearson correlation coefficient was calculated for each rater between evaluation 1 and 2 (INTERrater reliability) for the individual subsites, the entire face, and for the overall stage using Microsoft Excel 2013. A Pearson correlation coefficient was also calculated for each total score and stage comparing each rater on a head to head basis (INTERrater reliability) for time 1 and 2. Values greater than 0.6 are considered to be high correlation [7].
RESULTS
| Rater | |||||
| Subsite | 1 | 2 | 3 | 4 | Average |
| FH | ?0.81 (0.56-0.92) | ?0.73 (0.42-0.89) | ?0.70 (0.37-0.87) | ?0.83 (0.61-0.93) | 0.77 |
| Jowls | ?0.77 (0.50-0.90) | ?0.64 (0.27-0.84) | ?0.78(0.51-0.91) | ?0.87 (0.69-0.95) | 0.77 |
| ML/MAR | ?0.77 (0.50-0.90) | ?0.62 (0.24-0.83) | 0.44 (0-0.74) | ?0.80 (0.55-0.92) | 0.63 |
| Neck | ?0.85 (0.65-0.94) | ?0.89 (0.74-0.96) | *0.54 (0.13-0.79) | ?0.90 (0.76-0.96) | 0.8 |
*p < 0.05
?p < 0.01
| Rater | ||||
| 1 | 2 | 3 | 4 | Average |
| ?0.80 (0.55-0.92) | ?0.63 (0.26-0.84) | ?0.64 (0.27-0.84) | ?0.68 (0.34-0.86) | 0.69 |
Note: Table 4 represents the Pearson correlation based on the stage for each rater between time 1 and 2 and includes the 95% confidence interval.
*p < 0.05
?p < 0.01
The average INTERrater Pearson correlation for time 1 is 0.71 and for time 2 is 0.62 with an average of times 1 and 2 being 0.66. The scores comparing each examiner to the other examiners at time 1 and then time 2 is represented in table 5.
| 2-Jan | 3-Jan | 4-Jan | 3-Feb | 4-Feb | 4-Mar | Average | |
| Time 1 | ?0.62 (0.24-0.83) | ?0.66 (0.31-0.85) | ?0.69 (0.36-0.87) | ?0.60 (0.21-0.82) | ?0.84 (0.63-0.93) | ?0.69 (0.36-0.87) | 0.71 |
| Time 2 | ?0.66 (0.31-0.85) | ?0.73 (0.42-0.89) | ?0.70 (0.37-0.87) | *0.48 (0.05-0.76) | *0.48 (0.05-0.76) | ?0.68 (0.34-0.86) | 0.62 |
*p < 0.05
? p < 0.01
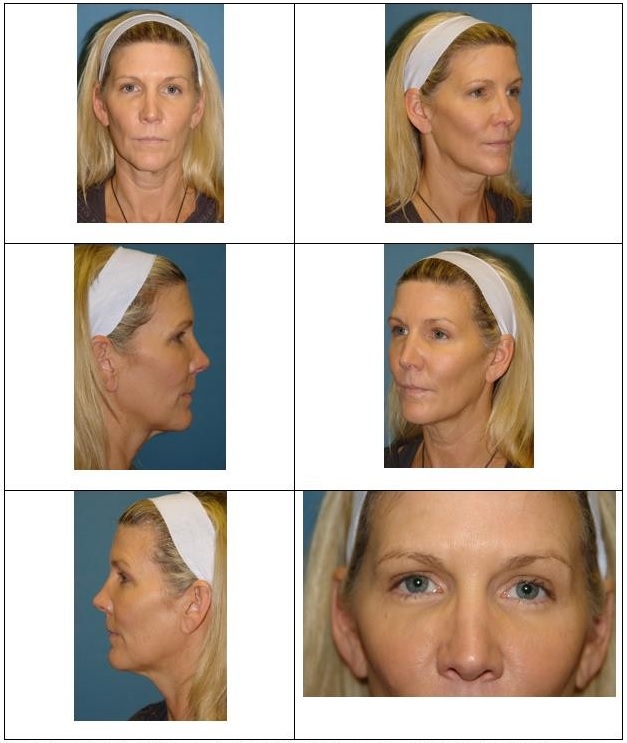

Figure 4: This patient was universally selected as a stage IV. Her average score for her forehead is 2.8 (range 2-4), jowls is 2.625 (range 2-3), melolabial fold/marionette lines is 2.25 (range 2-3), neck is 3.25 (range 2-4), and overall score is 10.875 (range 9-13).
DISCUSSION
This work is the next step in creating a more extensive algorithm for facial rejuvenation. It only evaluated the forehead, cheek, and neck. The rationale was that these areas had validated scales based on objective criteria that had been developed through joint collaboration between various aesthetic specialists including dermatologists, oculoplastic surgeons, and plastic surgeons at interdisciplinary and international conferences. The collaboration used to create these scales indicates both an applicability and usability among various specialties [4-7].
Just as the scales were shown to have high correlation levels in the original research, so did this study. A Pearson correlation coefficient greater than 0.6 is considered to have high correlation [7]. To assess the reliability of both the subscales and the stage, patients were assessed by four facial plastic surgeons, at least 30 days apart. The highest average degree of correlation was found in the neck (0.8 range: 0.54-0.90), followed by the forehead (0.77 range: 0.70-0.83) and jowls (0.77 range: 0.64-0.87), and finally the melolabial fold and marionette lines (0.63 range: 0.44-0.80).
The neck likely had the highest correlation given its ease of evaluation with a profile view. The forehead also had a high degree of correlation, which was better than that seen in the original studies (Pearson correlation coefficients: 0.47-0.51). This compares to the dynamic forehead rhytids evaluation in the original studies showing scores of 0.67 at time 1 and 0.65 at time 2 [4]. In this evaluation the brow position and forehead rhytids were grouped together and not analyzed separately. Evaluators were instructed if there was a discrepancy in the score or asymmetry between the sides to use the more severe aging scale. For example, if the static rhytids were a 2 and the brow position a 3 then the forehead was rated as a 3. This likely improved the correlation among the evaluators by being able to use multiple factors to evaluate and settling on the most severe sign of aging. Nevertheless, the results in the original study and the current one show a high degree of INTRArater reliability. The purpose of this study was not to further validate the results of the previous studies but rather to help validate the McCollough Facial Rejuvenation System as a foundation upon which an algorithmic approach will be established. The stages that were created were based on the descriptions previously published for each stage matched to the point values given in each subscale as seen in table 1 [1]. As can be seen in table 4 there was also a high degree of INTRArater reliability for staging of the patients (average 0.69, range 0.64-0.80). Furthermore, as can be seen in table 5 there is also a high degree of INTERrater reliability for staging the patients with an average at time 1 of 0.71 (range: 0.60-0.84) and at time 2 of 0.62 (range 0.48-0.73).
It is the expectation that the McCollough Facial Rejuvenation System Condition-Specific Algorithm can be more applicable to the practicing aesthetic surgeon by proving its validity. The previously described condition specific algorithms were much more detailed than the one presented here [1,2]. The reasoning for this is to begin the validation process of the staging system by limiting its scope. Once each section of the staging process has been validated it can be further applied to create an overall condition specific treatment algorithm. Furthermore, the subsites chosen are those most frequently addressed at the time of what has traditionally been referred to as a surgical rhytidectomy, namely, the forehead, cheek, and neck. The temple area has been indirectly validated within the scope of forehead as brow position was included in this subscale.
Overall this study confirms the reliability of the staging system at least in its evaluation of the forehead, cheek, and neck. The evaluators included those in large academic institutions and those in private practice. The evaluators span the generations of facial plastic surgeons from one of the founding members of the specialty to one of its newest members. Even with diverse degrees of experience, the evaluators applied similar scores regarding the overall stage of facial aging using the objective criteria, both descriptive and photo documentation, provided within. The senior author interpreted this commonality as a step toward establishing a language by which facial plastic surgeons in the future will be better able to communicate ideas and ideals.
By providing this validation it is hoped that it can lay the foundation for a broader discussion on facial analysis and provide a means of comparing techniques and outcomes based on the severity of the aging process.
CONCLUSION
REFERENCES
- EG M (2011) The McCollough Facial Rejuvenation System: A Condition-Specific Classification Algorithm. Facial Plast Surg 27: 112-123.
- McCollough EG, Ha CD (2012) The McCollough Facial Rejuvenation System: Expanding the Scope of a Condition-Specific Algorithm. Facial Plast Surg 28: 102-115.
- Carruthers A, Carruthers J (2010) A validated facial grading scale: the future of facial ageing measurement tools? J Cosmet Laser Ther 12: 235-241.
- Flynn TC, Carruthers A, Carruthers J, Geister TL, Görtelmeyer R, et al. (2012) Validated Assessment Scales for the Upper Face. Dermatol Surg 38: 309-319.
- Narins RS, Carruthers J, Flynn TC, Geister TL, Görtelmeyer R, et al. (2012) Validated assessment scales for the lower face. Dermatol Surg 38: 333-342.
- Sattler G, Carruthers A, Carruthers J, Flynn TC, Geister TL, et al. (2012) Validated assessment scale for neck volume. Dermatol Surg 38: 343-350.
- Carruthers J, Flynn TC, Geister TL, Görtelmeyer R, Hardas B, et al. (2012) Validated assessment scales for the mid face. Dermatol Surg 38: 320-332.
Citation: Guy WM, Rihani J, Brissett AE, Fedok F, McCollough EG (2016) Establishing Objectivity in the McCollough Facial Rejuvenation System. J Otolaryng Head Neck Surg 2: 004.
Copyright: © 2016 Marshall Guy W, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.