Journal of Reproductive Medicine Gynaecology & Obstetrics Category: Medical
Type: Case Report
Right Congenital Diaphragamatic Hernia with a Sac - A Case Report
*Corresponding Author(s):
Cátia Denise Ferreira RodriguesDepartment Of Obstetrics And Gynecology, Centro Hospitalar De Entre O Douro E Vouga, EPE, Aveiro, Portugal
Tel:+351 915002000,
Email:rodrigues_catia@hotmail.com
Received Date: Oct 17, 2018
Accepted Date: Nov 20, 2018
Published Date: Dec 04, 2018
Abstract
Congenital Diaphragmatic Hernia is a defect in the development of the diaphragm that allows the herniation of the abdominal viscera to the thoracic cavity. We intend to describe the case of a primigravida with 32 years with the diagnosis of fetal right congenital diaphragmatic hernia after the morphological ultrasound in the second trimester. Fetal magnetic resonance imaging confirmed this diagnosis, suggesting the presence of a herniac sac. Although adverse post-natal outcomes are more frequent and severe in cases of right CDH, the presence of the herniac sac is considered a predictor of better prognosis, as in the present case.
Keywords
Congenital diaphragmatic hernia; Fetal MRI; Prenatal diagnosis; Ultrasound
INTRODUCTION
Congenital Diaphragmatic Hernia (CDH) results from a defect in the development of the diaphragm that allows the herniation of the abdominal viscera to the thoracic cavity [1]. This partial or complete defect of the diaphragm frequently conditions the occurrence of pulmonary hypoplasia [2,3]. In very few cases, the defect is not a hole but a thinning or incomplete muscularization of the diaphragm, which is generally referred to as sac-type CDH.
The incidence of CDH is about 1 in 3000 - 5000 live births and most cases are isolated [1]. Associations with genetic, chromosomal or structural anomalies occur in about 30% of cases and heavily impact on the overall prognosis [2]. Pulmonary compression caused by abdominal viscera is responsible for hypertension and pulmonary hypoplasia, both by mechanical effect as by intrinsic changes that affect the normal development of the lung [3,4]. The most frequently affected side is the left (approximately 80-85% of cases) being rare the bilateral herniation [3,4]. The diagnosis of CDH is made by ultrasound, usually after 24 weeks of gestation. Fetal Magnetic Resonance Imaging (MRI) may be useful when there is doubt in the diagnosis or to optimize the fetal prognosis [1,4]. Despite advances in neonatal intensive care, CDH associated mortality remains high, ranging from 30 to 50% [5].
The incidence of CDH is about 1 in 3000 - 5000 live births and most cases are isolated [1]. Associations with genetic, chromosomal or structural anomalies occur in about 30% of cases and heavily impact on the overall prognosis [2]. Pulmonary compression caused by abdominal viscera is responsible for hypertension and pulmonary hypoplasia, both by mechanical effect as by intrinsic changes that affect the normal development of the lung [3,4]. The most frequently affected side is the left (approximately 80-85% of cases) being rare the bilateral herniation [3,4]. The diagnosis of CDH is made by ultrasound, usually after 24 weeks of gestation. Fetal Magnetic Resonance Imaging (MRI) may be useful when there is doubt in the diagnosis or to optimize the fetal prognosis [1,4]. Despite advances in neonatal intensive care, CDH associated mortality remains high, ranging from 30 to 50% [5].
CASE DESCRIPTION
We present the case of a 32-year-old primigravida with a history of uterine malformation - agenesis of the right uterine component with cervical septation and normal vagina. Pregnancy surveillance was uneventful. Early combined screening was negative and there were no ultrasound abnormalities in the first trimester. She performed a morphological ultrasound at our institution at 20 weeks, which showed no alterations in the echo anatomy. A new fetal ultrasound at 27 weeks revealed a communication between the abdominal and thoracic cavity. It was a right diaphragmatic hernia measuring 37x32 mm, with vascularization from the portal system, suggesting the presence of hepatic intrathoracic contents (Figures 1 and 2). It was also observed levocardia and displacement of the right lung in the superior direction, due to the herniated content. The karyotype was normal, 46, XY.
 Figure 1: Presence of ascites in the right hemithorax.
Figure 1: Presence of ascites in the right hemithorax. Figure 2: Vascularization from the portal system.
Figure 2: Vascularization from the portal system.Fetal MRI confirmed a massive right CDH that contained the right hepatic lobe surrounded by significant amount of fluid. This defect was associated with a left deviation of the mediastinum and a significant decrease of the right lung area, with about 4cc (Figure 3). The left lung maintained structure and volume preserved. Given the risk of need for postnatal surgical treatment the pregnant woman was transferred to a center with differentiated perinatal support. Delivery occurred at 37 weeks after premature rupture of membranes, resulting in a newborn male with 2860g and Apgar scores of 8 and 9 at 1 and 5 min, respectively.
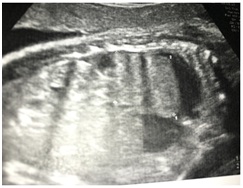 Figure 3: Right lung hypoplasia.
Figure 3: Right lung hypoplasia.On the 7th day of life the newborn was submitted to surgery, with a thoracotomy approach, to reduce the herniated viscera and to close the diaphragmatic defect. The surgery was uneventful and confirmed the presence of a hernia sac, previously suggested by the MRI. The newborn was discharged two weeks after surgery. After a year of surveillance in Pediatric consultation the child was discharged, with no need for further medical care.
DISCUSSION
The presence of an intrathoracic mass in the fetus may mean CDH, congenital cystic adenomatoid malformation, bronchopulmonary sequestration or bronchogenic cyst. All these malformations can result in pulmonary hypoplasia secondary to the mass effect [3,4]. CDH is the herniation of abdominal viscera to the fetal chest cavity due to a defect in the diaphragm. Although rare, CDH is the most frequent deformity of the diaphragm, occurring in about 1 in 3000 - 5000 live births [1]. Usually the diaphragmatic defect is posterolateral (Bochdalek) but may be retrosternal (Morgagni) or, rarely, central [3].
According to the most recent reviews, right CDH accounts for 8% to 21% of all CDH cases [1]. Right CDH occurs through the defect resulting from failure of the anterior pleuroperitoneal membrane to fuse with the sternum and costal cartilages during embryogenesis. The defect on the right is more difficult to diagnose because the heart remains on the left, the stomach maintains its normal position and the liver can easily be mistaken for the lung. The right CDH is suggested by the direction of portal vein flow, presence of as cites in the chest, or presence of gallbladder in the thoracic cavity. There are several theoretical explanations suggest that impact of right CDH might be worse. First, right lung normally accounts for 57% of total fetal lung volume and any compromise on its development may have a larger clinical impact. Second liver herniation through diaphragm is more frequently seen in right-sided defects, because of anatomic adjacency of the right lobe [6].
The most common forms of CDH correspond to a direct communication between the abdominal cavity and the thoracic cavity. Anatomically a hernial sac is a plueroperitoneal sac that covers and delimits the herniated contents in the thorax. The presence of this feature was reported in about 20% of the cases. Currently there is only one study that evaluated the prognostic value of the sac. This study concluded that in these situations there is greater preservation of lung volume and consequent better neonatal prognosis [7]. After the diagnosis the conduct should include a careful morphological ultrasound, a fetal echocardiogram and the cytogenetic study [7].
Although the ultrasound is the method of choice in pregnancy, fetal MRI is increasingly used. In the cases of CDH, MRI easily allows the distinction between liver, lung and intestine, as well as the relation between the liver and the diaphragm and the estimation of the remaining lung volume [8]. The most relevant prenatal prognostic factors are the value of the Lung-to-Head Ratio (LHR) and the presence of intrathoracic liver [9,10]. Current studies are controversial in relation to the severity of right CDH compared to left CDH cases, and it is not clear whether it is associated with higher mortality [11].
In most centers the treatment remains postnatal. The mean age for surgery is controversial and dependent on the postnatal evaluation, however it is agreed that the surgery should be performed after cardiopulmonary stabilization. Congenital diaphragmatic hernia mortality remains high. However in cases of isolated CDH the survival rate may reach 78% [5].
According to the most recent reviews, right CDH accounts for 8% to 21% of all CDH cases [1]. Right CDH occurs through the defect resulting from failure of the anterior pleuroperitoneal membrane to fuse with the sternum and costal cartilages during embryogenesis. The defect on the right is more difficult to diagnose because the heart remains on the left, the stomach maintains its normal position and the liver can easily be mistaken for the lung. The right CDH is suggested by the direction of portal vein flow, presence of as cites in the chest, or presence of gallbladder in the thoracic cavity. There are several theoretical explanations suggest that impact of right CDH might be worse. First, right lung normally accounts for 57% of total fetal lung volume and any compromise on its development may have a larger clinical impact. Second liver herniation through diaphragm is more frequently seen in right-sided defects, because of anatomic adjacency of the right lobe [6].
The most common forms of CDH correspond to a direct communication between the abdominal cavity and the thoracic cavity. Anatomically a hernial sac is a plueroperitoneal sac that covers and delimits the herniated contents in the thorax. The presence of this feature was reported in about 20% of the cases. Currently there is only one study that evaluated the prognostic value of the sac. This study concluded that in these situations there is greater preservation of lung volume and consequent better neonatal prognosis [7]. After the diagnosis the conduct should include a careful morphological ultrasound, a fetal echocardiogram and the cytogenetic study [7].
Although the ultrasound is the method of choice in pregnancy, fetal MRI is increasingly used. In the cases of CDH, MRI easily allows the distinction between liver, lung and intestine, as well as the relation between the liver and the diaphragm and the estimation of the remaining lung volume [8]. The most relevant prenatal prognostic factors are the value of the Lung-to-Head Ratio (LHR) and the presence of intrathoracic liver [9,10]. Current studies are controversial in relation to the severity of right CDH compared to left CDH cases, and it is not clear whether it is associated with higher mortality [11].
In most centers the treatment remains postnatal. The mean age for surgery is controversial and dependent on the postnatal evaluation, however it is agreed that the surgery should be performed after cardiopulmonary stabilization. Congenital diaphragmatic hernia mortality remains high. However in cases of isolated CDH the survival rate may reach 78% [5].
CONCLUSION
Although the diagnosis is made by ultrasound, fetal MRI plays an important role in the prenatal study, particularly in the right CDH. This exam has great accuracy in the assessment of lung volume, which is an important prognostic factor. Right CDH is a rare variant of CDH with the particularity of representing a greater diagnostic challenge. However, prenatal diagnosis is essential to optimize labor and postnatal prognosis.
REFERENCES
- Hedrick HL, Crombleholme TM, Flake AW, Nance ML, von Allmen D, et al. (2004) Right congenital diaphragmatic hernia: Prenatal assessment and outcome. J Pediatr Surg 39: 319-323.
- Enns GM, Cox VA, Goldstein RB, Gibbs DL, Harrison MR, et al. (1998) Congenital diaphragmatic defects and associated syndromes, malformations, and chromosome anomalies: A retrospective study of 60 patients and literature review. Am J Med Genet 79: 215-225.
- Gratacós E, Martinez R (2018) Congenital diaphragmatic hérnia. Isuog, London, UK.
- Santos E, Ribeiro S (2008) [Hérnia diafragmática congénita - artigo de revisão]. Acta Obstet Ginecol Port 2: 25-33.
- Stege G, Fenton A, Jaffray B (2003) Nihilism in the 1990s: The true mortality of congenital diaphragmatic hernia. Pediatrics 112: 532-535.
- Bidiwala A, Bishara J, Burjonrappa S (2016) Right sided congenital diaphragmatic hernia: Diagnostic, prognostic and therapeutic implications. In: Collins R (ed.). Incisional and Congenital Diaphragmatic Hernia (CDH): Risk Factors, Management and Outcomes. Nova Science Publishers, Inc., New York, USA. Pg no: 113-130.
- Spaggiari E, Stirnemann J, Bernard JP, De Saint Blanquat L, Beaudoin S, et al. (2013) Prognostic value of a hernia sac in congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 41: 286-290.
- Gorincour G, Bouvenot J, Mourot MG, Sonigo P, Chaumoitre K, et al. (2005) Prenatal prognosis of congenital diaphragmatic hernia using magnetic resonance imaging measurement of fetal lung volume. Ultrasound Obstet Gynecol 26: 738-744.
- Rottier R, Tibboel D (2005) Fetal lung and diaphragm development in congenital diaphragmatic hernia. Semin Perinatol 29: 86-93.
- Fauza DO, Wilson JM (1994) Congenital diaphragmatic hernia and associated anomalies: Their incidence, identification, and impact on prognosis. J Pediatr Surg 29: 1113-1117.
- Jani JC, Benachi A, Nicolaides KH, Allegaert K, Gratacós E, et al. (2009) Prenatal prediction of neonatal morbidity in survivors with congenital diaphragmatic hernia: A multicenter study. Ultrasound Obstet Gynecol 33: 64-69.
Citation: Rodrigues CDF, Cunha SB, Reis IF, Pinto MA, Teles TP (2018) Right Congenital Diaphragmatic Hernia with Sac – A Case Report. J Reprod Med Gynecol Obstet 3: 014.
Copyright: © 2018 Cátia Denise Ferreira Rodrigues, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2024, Copyrights Herald Scholarly Open Access. All Rights Reserved!