Factors Influencing Hemodialysis Patients Survival Using Frailty Models
*Corresponding Author(s):
Mohammad Mehdi DindarlooEpidemiology And Biostatistics Department, Health Faculty, Mazandaran University Of Medical Science, Sari, Iran
Jamshid Yazdani-Charati
Professor Of Biostatistics, Epidemiology And Biostatistics Department, Health Faculty, Health Science Research Center, Mazandaran University Of Medical Science, Sari, Iran
Email:Jamshid.charati@gmail.com
Abstract
Background and objection: Hemodialysis is the most common renal replacement therapy in patients with End Stage Renal Disease (ESRD). This study investigated the 5-year survival rate of hemodialysis patients admitted to Imam Khomeini and Fatima Zahra Hospitals in Sari.
Materials & Methods: This study was performed on 335 patients on hemodialysis referring to Imam Khomeini and Fatima Zahra Hospitals from November 2008 to November 2013. To investigate the factors influencing the patients' survival rate, we used Cox model and Frailty model and compared these models efficiency, we also applied the Akaikie information criterion and the residuals review. All calculations have been performed with SPSS version 20 & STATA version 8 and the significance level was 0.05.
Findings: The results of this study showed that applying the Kaplan– Meier method to determine one, three and five year’s survival rates for hemodialysis patients were 74.9%, 53.2% and 20.4%, respectively. The mean survival time was 37.241 months. In the final model, in multivariate analysis of the gamma frailty model, the variables as age, education, marital status, diabetes, Kidney stone & obstructions, the clinic, the mean serum albumin and urea have been identified as the most important predictors in hemodialysis patients' survival (p < 0.05).
Conclusion: According to the results of the frailty model fitness, the hemodialysis patients having the same explanatory variables also have different risk of death. Giving the Akaikie information criterion and the residuals review, the Weibull model with gamma frailty is more efficient than the Cox model and it has good fitness to the data.
Keywords
Cox proportional hazards model; Gamma frailty model; Hemodialysis; Kaplan-Meier model; Survival analysis
Introduction
Renal natural performances including various cellular processes maintain homeostasis (internal body condition balance). Disorder in every processes create a set of abnormal states that may harm health [1]. Irreversible loss of renal function lasting more than 3 months is called chronic renal failure and its advanced stage requiring dialysis or transplant for survival is known as End Stage Renal Disease (ESRD) [2]. Apart from common therapies like kidney replacement ,hemodialysis is considered the dominant method in most of ESRD patients [3] and dialysis is a life-saving treatment for patients with end-stage renal disease [4]. Regarding the extensive access to dialysis, hundreds of thousands of the ESRD patients' Lives got longer. Globally, the ESRD-stricken patients' death rate in Europe and Japan is relatively insignificant while in the developing countries, this rate is very high due to limitation in accessing hemodialysis. In the U.S.A, the dialysis patients' death rate is almost 18-20% and their 5-year survival rate is about 30-35 % [1]. Based on the U.S renal information system, around 90% of chronic renal failure patients are under hemodialysis therapy and among 92% of the hemodialysis patients, this method is preferred [5].
Survival analysis is used in various fields for data analysis existing between the event incidence or the conditions & situations changing time [6]. Temporal observations resulting from these studies along with the censored data are called "survival data" and the set of statistical methods for their analysis is termed "survival analysis" [7]. Censor happens when we have truncated data about survival time of some of the study subjects [8]. In some studies, there may be some unknown factors other than the covariates seriously influencing survival time distribution and subsequently, hazard function. However, due to being unknown and or disability to measure them, we are not able to include them in regression model (like unknown genetic or environmental factors). In the general state, if a factor influences response variable, it is necessary to obtain its value for every subject and include it in the model as a covariate. But if such action is impossible, the variations from hazard function that could be explained & decreased through the existing related factor are summed with error term and as a result that That will increase hazard function variations relative to the state that the considered factor exists in the model. The increased variations result in hazard function change and cause the regression coefficients change and approach zero numerically and in general state, they Will obtain skewed & misleading estimators from the regression parameters. Unknown risk factors in the univariate survival analysis lead to increase heterogeneity in survival time and the multivariate survival analysis; they create correlation between intragroup survival times. In both of the mentioned states, estimating the parameters by using regular model of Cox Proportional Hazard Model (CPHM) gets skewed and misleading .But by applying Frailty Models (FM), it is possible to remove the imperfection [7,9,10].
This study aims to investigate the factors influencing hemodialysis patients' survival using frailty model and to determine survival rate and such patients' risk factors .In addition, comparing the parameters estimate in Cox & Frailty models despite the existence of unknown risk factors shows the effect of utilizing frailty effect on the model fitness improvement and the estimators' accuracy increase.
Materials And Methods
This study was approved by the Clinical Research Ethics Committee of the Mazandran University of Medical Science. All procedures adhere to the Declaration of Helsinki. This is a retrospective cohort study of the hemodialysis patients referring to Sari-based Imam Khomeini and Fatima Zahra Hospitals from November 2008 to November 2013 and they have files in the hospitals archives. In this study, sampling has been done by census and the patients' information has been collected via checklist whose validity has been confirmed by this plan statistical & medical counselor. Some of the information has been gathered by calling and the patients' survival time has been estimated in months. In the present research, the number of the patients on hemodialysis has been 335 and in the study, the subjects alive (survived) at the end of the study and the ones lost to follow-up have been considered the right censor. The covariates in this research are employed to get the hemodialysis patients' survival prognostic factors including gender, age(years), education level, marital status, employment, smoking record, disease leading to dialysis (diabetes, hypertension, Kidney stone & obstructions, Polycystic Kidney Disease (PKD), congenial diseases, uncertain, the other) the disease leading to dialysis diagnosis age(years), General Health Questionnaire (GHQ), cardiovascular disease affliction, dialysis initiation age (years), the mean serum albumin(mg/dL),mean serum creatinine(mg/dL),mean urea(mg/dl) and clinic.
If the covariates are known, they can be applied in analysis; however, it is almost impossible for it to include all important risk factors, perhaps because we have very little information at individual levels. Besides, maybe it is because we haven’t risk factors relationship. Under such conditions, it is useful to take two variability sources in the data length into account: the observable risk Factors variability was theoretically predictable and the heterogeneity due to the unknown & unpredictable risk covariates not being predicted theoretically. The unobservable risk factors expressed by a synthetic variable called frailty which is a random one tracks down several distributions [11]. If we take Z as the known variables vector and the unknown variables influencing hazard function in both, then the real model of Cox Proportional at time t will be in the form of λ0(t)exp(β'zi+Ψ'w). Since W is unknown or immeasurable, we assume Expo (Ψ'w) random and take it as random effect or frailty effect Y and put in the model as the following. This model shows that risk at time t is as it follows: The above model is known as the modified Cox model or the Survival Frailty model [12].
The above model is known as the modified Cox model or the Survival Frailty model [12].
The significant issue in frailty models is choosing the frailty distribution. because of simplifying the estimations and since the frailty model stands for the relative risk of unknown factors ,in most cases ,the mean frailty effect distribution is assumed one [13]. In this study of the frailty component has gamma distribution with mean 1 and variance θ.
Weibull distribution is a very flexible model for the survival time data. Weibull distribution survival function S(x) = exp[- λxα] is for x > 0. Here λ > 0 is a scale parameter and α > 0 is a shape parameter [14].
To evaluate the comparison of the models used in this study, we have employed Akaike Information Criterion (AIC).The formula for statistical AIC index is:
 In this relation P is the parameters number, K (constant factor) for Weibull model equals 2. AIC is a parameter for the statistical models fitness and denotes which model has better fitness on data [14]. Lower AIC value will show the better fitness of the model. The model execution & data analysis have been done in STATA software version 8 and the significance level has been considered 0.05.
In this relation P is the parameters number, K (constant factor) for Weibull model equals 2. AIC is a parameter for the statistical models fitness and denotes which model has better fitness on data [14]. Lower AIC value will show the better fitness of the model. The model execution & data analysis have been done in STATA software version 8 and the significance level has been considered 0.05.
Findings
In the present study, out of 335 patients followed up, 168 (50.1%) died and 167(49.9%) have been introduced as censor. In terms of gender incidence, 45.4 %( 152) of the patients were women and 54.6% (183) were men (Table 1). One, two, three, four & five year survival probability of the study hemodialysis patients has been 74.9%,63.4%,53.2%,44.4% & 20.4%,respectively. The average lifetime of patients has been achieved 37.241 months with confidence level around 95 %( 34.51, 39.97).
|
Variable |
Man (183=n) |
Woman (152=n) |
Total |
P- value |
|
S.D±Mean |
Patients(n=335) |
|||
|
age |
15.43 ± 62.04 |
62.01 ±15.91 |
15.63±62.03 |
0.988 |
|
disease diagnosis age |
17.55 ± 48.81 (84=n) |
19.42 ± 47.28 (71=n) |
18.39 ± 48.11 (155=n) |
0.608 |
|
dialysis initiation age |
16.25 ± 59.34 |
16.81 ± 59.22 |
16.48 ±59.28 |
0.951 |
|
mean serum albumin |
0.43 ± 4.25 |
0.42±4.25 |
0.43 ± 4.25 |
0.946 |
|
mean serum creatinine |
3.77 ± 8.58 |
2.59 ± 6.79 |
3.36 ± 7.72 |
0.003 |
|
urea mean |
44.43 ± 99.51 |
36.11±92.73 |
40.93 ± 96.44 |
0.21 |
|
Education status |
||||
|
Uunder diploma |
27.5%(92) |
23.6% (79) |
51%(171) |
0.421 |
|
diploma& Higher |
27.2%(91) |
21.8%(73) |
49% (164) |
|
|
Marital status |
||||
|
Single |
5.1%(17) |
5.1%(17) |
10.1%(34) |
0.347 |
|
Married |
49.6%(166) |
40.3%(135) |
89.9%(301) |
|
|
Employment |
||||
|
Housewife & Jobless |
5.1%(17) |
16.9% (147) |
49%(164) |
0 |
|
Office worker |
7.5% (25) |
0.9%(3) |
8.4%(28) |
|
|
Farmer |
11% (37) |
0%(0) |
11%(37) |
|
|
Retired & Other |
31% (104) |
0.6%(2) |
31.6%(106) |
|
|
Smoking Record |
||||
|
No |
31.3%(105) |
43%(144) |
74.3%(249) |
0 |
|
Yes |
23.3%(78) |
2.4%(8) |
25.7%(86) |
|
|
Disease leading to dialysis |
||||
|
Diabetes |
23.6%(79) |
24.5%(82) |
48.1%(161) |
0.098 |
|
Hypertension |
8.1%(27) |
7.5%(25) |
15.5%(52) |
|
|
Kidney stone & obstructions |
3.6%(12) |
0.9%(3) |
4.5%(15) |
|
|
Polycystic kidney disease & Congenital disease |
2.4%(8) |
0.9%(3) |
3.3%(11) |
|
|
unknown |
11%(37) |
9.3%(31) |
20.3%(68) |
|
|
Other |
6%(20) |
2.4%(8) |
8.4%(28) |
|
|
Cardiovascular diseases |
||||
|
No |
31.1%(101) |
23.9%(80) |
54% (181) |
0.36 |
|
yes |
24.5%(82) |
21.5%(72) |
46.8%(154) |
|
|
General Health Questionnaire (GHQ) |
||||
|
Less than or equal 3 |
29.5%(33) |
17.9%(20) |
47.3%(53) |
0.252 |
|
More than 3 |
28.6%(32) |
24.1%(27) |
52.7%(59) |
|
|
Clinic |
||||
|
Imam Khomeini |
31.9% (107) |
27.8%(93) |
59.7%(200) |
0.348 |
|
Fatima Zahra Hospitals |
22.7%(76) |
17.6%(59) |
40.3%(135) |
Table 1: The hemodialysis patients' specifications by gender separation.
|
Variable |
Hazard ratio (HR) ** |
P-Value |
AIC |
|
Age |
1.00 |
0.413 |
1382.35 |
|
Marital status |
1.76 |
0.026* |
1381.72 |
|
Employment |
1.03 |
0.407 |
1385.34 |
|
Smoking record |
1.48 |
0.025* |
1381.24 |
|
Diabetes |
1.33 |
0.090 |
1383.14 |
|
Hypertension |
0.63 |
0.050* |
1381.81 |
|
Kidney stone & obstructions |
0.47 |
0.142 |
1383.28 |
|
Disease diagnosis age |
1.00 |
0.757 |
733.36 |
|
Cardiovascular diseases |
1.77 |
0.001* |
1374.50 |
|
Dialysis initiation age |
1.00 |
0.396 |
1385.30 |
|
Mean serum albumin |
0.38 |
0.00* |
665.45 |
|
Mean serum creatinine |
1.06 |
0.207 |
691.36 |
|
Mean urea |
0.67 |
0.020* |
674.04 |
|
Clinic |
0.72 |
0.061 |
1382.54 |
Table 2: Cox regression model results in the hemodialysis patients 'survival univariate analysis P-Value < 0.05 ** Hazard Ratio-HR*.
|
Variable |
Standardized regression coefficient (βi*) |
Hazard ratio exp(βi) |
P-Value |
Confidence level 95% |
|
Age |
0.77 |
1.01 |
0.488 |
(1.04 , 0.98) |
|
Marital status |
1.99 |
3.61 |
0.102 |
(16.82 , 0.78) |
|
Employment |
0.79 |
0.92 |
0.444 |
(1.13 , 0.76) |
|
Smoking record |
1.05 |
1.56 |
0.288 |
(3.56 , 0.68) |
|
Diabetes |
3.07 |
1.19 |
0.743 |
(3.33 , 0.42) |
|
Hypertension |
1.06 |
0.56 |
0.289 |
(1.63 , 0.19) |
|
Kidney stone & obstructions |
1.83 |
5.22 |
0.070 |
(31.17 , 0.87) |
|
Disease diagnosis age |
0.39 |
1.00 |
0.830 |
(1.04 , 0.97) |
|
Cardiovascular diseases |
1.12 |
1.54 |
0.315 |
(3.16 , 0.66) |
|
Dialysis initiation age |
0.89 |
0.99 |
0.626 |
(1.03 , 0.95) |
|
Mean serum albumin |
2.75 |
0.34 |
0.00* |
(0.68 , 0.17) |
|
Mean serum creatinine |
0.15 |
1.06 |
0.905 |
(2.81 , 0.40) |
|
Mean urea |
1.94 |
0.59 |
0.225 |
(1.38 , 0.25) |
|
Clinic |
3.59 |
4.01 |
0.045* |
(15.49 , 1.03) |
|
Akaikie information criterion
|
336.40 = AIC |
_ |
_ |
_ |
Table 3: Cox regression model results in the hemodialysis patients 'survival multivariate analysis P-Value < 0.05.
The issue that the variables as marital status, smoking record, hypertension, cardiovascular disease affliction and mean urea got meaningful in univariate analysis but not in multivariate analysis can be attributed to the correlation between the data. To remove the problem behind the correlation between the data, we have used standardized regression coefficients for data analysis. The standardized regression coefficients are calculated by this formula.
 Regarding the results gained in table 3, we perceive that the mean serum albumin variable effect size is -2.75 in terms of response variable variation speed (the patients' survival time) and the clinic variable effect is -3.59 in terms of response variable variation speed (the patients' survival time). With respect to the importance of the mean serum albumin in the hemodialysis patients' survival and the negative value of these two variables effect size and the relative hazard value related to them, it seems that the result of the obtained estimations are skewed and misleading. On the one hand, the variables as mean serum albumin and clinic getting meaningful in hemodialysis patients' survival using Cox regression model can be attributed to some unknown factors such as personal & environmental traits of the patient being special to the person and that they create a certain trait for the patient. In this case, to cope with such a phenomenon, we use frailty models [10].
Regarding the results gained in table 3, we perceive that the mean serum albumin variable effect size is -2.75 in terms of response variable variation speed (the patients' survival time) and the clinic variable effect is -3.59 in terms of response variable variation speed (the patients' survival time). With respect to the importance of the mean serum albumin in the hemodialysis patients' survival and the negative value of these two variables effect size and the relative hazard value related to them, it seems that the result of the obtained estimations are skewed and misleading. On the one hand, the variables as mean serum albumin and clinic getting meaningful in hemodialysis patients' survival using Cox regression model can be attributed to some unknown factors such as personal & environmental traits of the patient being special to the person and that they create a certain trait for the patient. In this case, to cope with such a phenomenon, we use frailty models [10].
The empirical hazard function curve indicates ascending risk. Considering the hazard function in survival univariate and multivariate data is positive, in both states it is essential to consider a positive distribution for frailty effect(13).Therefore, giving the hazard function curve shape(not estimated here), we can use Weibull distribution for data here [16]. Weibull model along with gamma frailty is considered as parametric model. Weibull distribution covers both qualitied like proportional hazards and Accelerated Failure Time (AFT) models is that the covariates effect is a multiple of survival time. In Weibull distribution AFT model, we show the obtained regression estimates as αj and call γi = exp(αi) as acceleration factor and show it as γi [17] whose value is more than 1 which results in longer survival time for the patient [18].Tables 4&5 showed the variables effect on the hemodialysis patients' death risk in univariate and multivariate analysis of frailty model. is observed as seen in univariate analysis, the variables such as marital status, smoking record, cardiovascular disease affliction, mean serum albumin and mean urea in univariate analysis had influenced the hemodialysis patients' survival chance.
|
Variable |
Standardized Regression Coefficient (αi*) |
Acceleration Factor γi = exp(αi) |
P-Value |
AIC |
|
Age |
0.31- |
0.99 |
0.407 |
657.96 |
|
Marital status |
0.84 - |
0.58 |
0.026* |
654.35 |
|
Employment |
0.40 - |
0.96 |
0.334 |
657.73 |
|
Smoking record |
0.93- |
0.67 |
0.020* |
653.41 |
|
Diabetes |
0.59- |
1.25 |
0.16 |
656.69 |
|
Hypertension |
1.45 |
1.46 |
0.084 |
655.43 |
|
Kidney stone & obstructions |
0.75 |
1.97 |
0.167 |
656.25 |
|
Disease diagnosis age |
0.13- |
1.00 |
0.781 |
376.19 |
|
Cardiovascular diseases |
1.48- |
0.56 |
0.000* |
646.22 |
|
Dialysis initiation age |
0.38- |
1.00 |
0.366 |
657.83 |
|
Mean serum albumin |
1.66 |
1.92 |
0.000* |
325.43 |
|
Mean serum creatinine |
0.51 |
1.22 |
0.198 |
344.65 |
|
Mean urea |
1.11 |
1.35 |
0.016* |
333.66 |
|
Clinic |
0.70 |
1.31 |
0.092 |
655.83 |
Table 4: Frailty model results in the hemodialysis patients 'survival univariate analysis P-Value < 0.05*.
|
Variable |
Standardized regression Coefficient (αi*) |
Acceleration factor γi = exp(αi) |
P-Value |
Confidence level 95% |
|
Age |
2.54- |
1.03 |
*0.039 |
(0.00,0.06) |
|
Marital status |
2.68- |
0.18 |
0.003* |
(-2.86, -0.59 |
|
Education |
2.37- |
0.40 |
*0.014 |
(-1.65, -0.19) |
|
Smoking record |
0.39 |
1.18 |
0.456 |
(-0.27, 0.61) |
|
Diabetes |
1.34- |
0.60 |
*0.031 |
(-0.98,-0.05) |
|
Kidney stone & obstructions |
-1.28 |
0.31 |
*0.003 |
(-1.93, -0.38) |
|
Disease diagnosis age |
0.03- |
1.00 |
0.958 |
(-0.01, 0.01) |
|
Cardiovascular diseases |
1.04- |
0.67 |
0.090 |
(-0.87, 0.06) |
|
Mean serum albumin |
1.45 |
1.78 |
0.005* |
(0.17, 0.98) |
|
Mean urea |
1.85 |
1.65 |
0.003* |
(0.17, 0.83) |
|
Clinic |
-1.69 |
0.52 |
*0.011 |
(-1.15, -0.15) |
|
Frailty variance |
=2.72 |
_ |
*0.009 |
(0.77, 9.65) |
|
AIC |
156.41 |
_ |
_ |
_ |
Table 5: The results of Weibull model parametric along with gamma frailty in the hemodialysis patients'survival multivariate analysis P-Value < 0.05*.
In the frailty model multivariate analysis which used stepwise method through eliminating the confounding effect and considering the AFT for coping with the unknown variables effect, the factors affecting the hemodialysis patients survival have been identified and the variables of age, marital status, diabetes, Kidney stone & obstructions, mean serum albumin, mean urea and clinic have been introduced as the variables which affecting the hemodialysis patients survival. In the fitted model, the frailty variance was obtained 2.72 (P-Value=0.009 the significance of frailty component variance in the model implies that the hemodialysis patients who has similar explanatory variables also have different death incidence risk. In other words, in addition to explanatory variables, some other factors affect death incidence which being peculiar to that person and create hazard function heterogeneity in that community. On the one hand, the variables got meaningful in the frailty model univariate analysis could get also meaningful in the frailty model multivariate analysis. In other hand in Cox model, such result wasn’t obtained and indicated the appropriate frailty model matched with data. As seen in tables 3&5, Weibull model along with gamma frailty has lower Akaike criterion value. Accordingly, it has better fitness to the data. In the Data of univariate analysis also the frailty model Akaike criterion value is more than half of the Cox model is almost half of the Cox model Akaike criterion value and this revealed the frailty model efficiency. However for the evaluation and comparison of the utilized models, Cox-Snell Residuals in the Cox & Weibull models along with gamma frailty have been applied. The corresponding lines with Cox-Snell Residuals are closer to the line in frailty model showing better fitness to the data of this model. These results are also consistent with Akaike criterion (Diagrams 1 & 2).
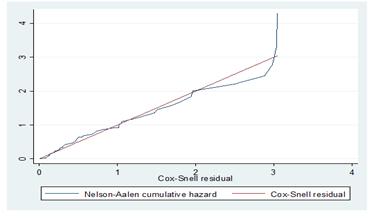 Diagram1: Cox -Snell Residuals in Cox model.
Diagram1: Cox -Snell Residuals in Cox model.
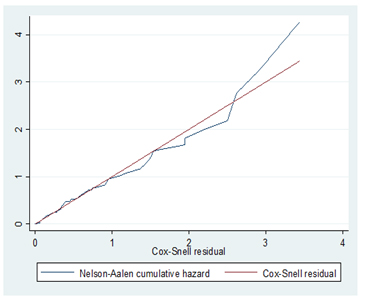 Diagram 2: Cox - Snell Residuals in Weibull model along with gamma frailty model.
Diagram 2: Cox - Snell Residuals in Weibull model along with gamma frailty model.
Discussion
The End Stage Renal Disease (ESRD) indicates a clinical condition as a result of kidneys disability the metabolic actions and create liquids & metabolites equilibrium in the body [19] and for patient surviving, the using of renal replacement therapy will be inevitable. Despite the geographical differences, hemodialysis is the most common therapy for ESRD [19]. The frailty model was first used by Clayton in 1987 and for patient surviving; the using of renal replacement therapy will be inevitable. The frailty models are relatively new models in survival and were broadly investigated in 1990 [7]. Utilizing the frailty component in Cox relative hazards model caused accurate estimation of regression coefficients and the patient’s personal traits effect is introduced into the model. In various studies, the frailty model has been applied to analyze data [21-23].
In this study, the gender ratio is 1.20 that is in line with the research by Argyropoulos et al. in the U.S (24)and in some studies, it is lower (25-28)and in some other ones, it is higher than the other (4, 5, 29). The average age of hemodialysis patients in this research was 62.04 ±15.43 and the highest age frequency was related to age group 61-80.Though,the Average age in the study by Jungers et al. in Paris, was 53.8±17.2 [30] and in the research by Ahuja et al. in the U.S , was 39.4±8.9 (26). About the disease lead dialysis diagnosis age in males and females, the maximum frequency was 41-60.and the patients dialysis initiation age, the maximum frequency was for 61-80 .The patients median survival time has been gained 44 months with 95% assurance (35.69, 52.30).While in Argyropoulos et al [24] study in the USA, the median survival time was obtained 48.4 month and in the research by Yeates et al [25] in Australia, the median survival time was gained 52.3 months.
In the present research, the average hemodialysis women patients' longevity is 39.34 ±2.12 months and it is 35.65 ±1.85 months for men. This result matches the research by Ahuja et al. in the U.S [26]. In this study, age has been identified as an important predictive factor for the hemodialysis patients' survival in this sense that Elderly ones were exposed to a tangible increase in their death risk due to the disease .These findings have been verified by many studies in this field [5,21,24,27,28,30-34]. In multivariate analysis, the age effect size on the response variable variation speed (the patients’ survival time) is -2.54. It means that for one year increase in the patients’ survival time, it decreases by 2.54 times. In the U.S.A, the main reason behind ESRD is diabetes mellitus and the second one is hypertension that based on the estimation, which created 28% of ESRD cases. In the present study, in the frailty model multivariate analysis, diabetes has been identified as an important predictive of the hemodialysis patients survival. The findings suggested that being afflicted by the diabetes decreases the hemodialysis patients’ survival time by 1.34 times. This finding has been consistent with many studies' results in this field [5,21,30,31,34]. One of the main Reasons of renal failure is the kidney arteries obstruction. In this study, the kidney stone and obstructions disease has been recognized as a significant predictive factor for the hemodialysis patients survival time .In fact, being afflicted by renal obstructions disease reduces the hemodialysis patients survival time by 1.28 times. This result also complies with the studies by Mousavi et al [35].
In addition, many studies have revealed that the mean low serum albumin is associated with lower survival [5,24,28,30,34]. In the current study, regarding the estimated parameter of the acceleration factor, the survival time of the hemodialysis patients with mean serum albumin higher than 4 is 1.78 times more than the hemodialysis patients whose mean serum albumin is less than 4. As a result, the mean serum albumin lower than 4 is one of the major reason of the hemodialysis patients deaths.
However the mean blood urea (the measured level before hemodialysis session) has also been introduced as one of the important predictive factors for the hemodialysis patients survival .Concerning the acceleration factor estimated parameter, the survival time of the hemodialysis patients with mean urea higher than 60 is 1.65 times than the hemodialysis patients with the mean urea less than 60.This result agrees with the research by liu et al [36]. Besides, in this study the demographic variables Such as marital status and education level have been recognized as the main predictive factors of the hemodialysis patients' survival. The effect size of marital status variable is -2.37.This matter can be attributed to the effect of marriage on the person's spirit and creating motivation in him/her for living and also family support and the spouse and children caring the patient's health. This result is in line with the studies conducted in this field [37]. On the one hand, the effect size of the variable namely education level is -2.37.This matter can be justified in the studying, knowledge and attention of the educated hemodialysis patients about taking care of themselves and following special diet and correct use of their medicine .This result is consistent with some studies in this area [38].
Another variable recognized as one of the important hemodialysis patients survival is clinic. The effect size of the variable clinic is -1.69.On the one hand, regarding the acceleration factor estimated parameter, the hemodialysis patients' survival time referring to Fatima Zahra Hospital dialysis ward is 0.52 times than that of the hemodialysis patients referring to Imam Khomeini Hospital. The reason behind it can be put in the difference between the various dialysis centers' facilities and health services, the dialysis center capacity, the dialysis adequacy, the dialyzers number and some other unknown factors .This finding matches with the research by Carvalho et al. [21,28].The main reason of the ESRD patients death under chronic dialysis is cardiovascular diseases (20).In this research also, cardiovascular disease is identified as one of the significant predictive factors of the hemodialysis patients survival both in Cox model univariate analysis and gamma frailty model univariate analysis that is compatible with many studies in this field [24,25,27,30,31,39].
The findings revealed that being afflicted by cardiovascular diseases decreases the hemodialysis patients survival time by 1.48 times. Also the acceleration factor rate of cardiovascular disease is 0.56 and since this rate is less than 1, It shows harmful exposure Smoking not only increases the renal disease risk, but also raises the deaths rate due to the heart stroke of the individuals suffering from chronic renal disease. In this research smoking has been recognized as one of the important predictive factors of the hemodialysis patients' survival both in Cox model univariate analysis and gamma frailty univariate analysis. The acceleration factor estimated parameter shows the hemodialysis patients' survival time with smoking record as 0.67 times than the ones with no smoking record .Thus the acceleration factor indicates the harmful exposure to smoking record. This finding coordinates with the study by Yeats et al [25]. The present study has some limitations too, that we can mention some such as the flaw in the patients' file and memory, their telephone number & addresses changing and not accessing them and in some cases, the patients or their families not willing to cooperate in answering the questions.
Conclusion
Regarding the achieved results from the frailty model fitness, the hemodialysis patients with similar explanatory variables have different death incidence hazard. Also in this study, with respect to the plan medical counselor's opinion, the results obtained from Weibull model along with gamma frailty model to determine the predictive factors of the hemodialysis patients’ survival conform to the scientific principles and it is practical for applied research cases.
Declaration
Ethical Approval and Consent to participate: The study protocol was following the Helsinki Declaration and was confirmed by the Ethics Committee of Mazandaran University of Medical Sciences (Approval Code: IR.MAZUMS.REC.1391.324). The participants were informed about the research objectives and an informed consent form was obtained from the subjects before starting the survey.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request to the corresponding author.
Competing interests
The authors hereby affirm that the manuscript is original, that all statements asserted as facts are based on authors' careful investigation and accuracy, that the manuscript has not been previously published in total or in part and has not been submitted or considered for publication in total or in part elsewhere. Each author acknowledges he/she has participated in the work substantively and is prepared to take public responsibility for the work and authors have no competing interest in the results of the article.
Funding
Not applicable.
Author's contribution
Conceptualization: JY, Methodology: JY, MM,MMD, Software: JY,MM,MMD,Validation: JY, Formal analysis: JY,MM,MMD,Investigation: JY, Resources: JY,MMD,Data curation: FE, Writing (original draft preparation): JY,MM,MMD, Writing (review and editing): JY, Visualization: JY, Supervision: JY, Project administration: JY, FE, Funding acquisition: JY.
Acknowledgement
Hereby we greatly appreciate all the patients participating in this study and sincere cooperation of the honored personnel of the hemodialysis wards of Imam Khomeini and Fatima Zahra Hospitals in Sari.
References
- Fauci, Braunwald, Kasper, Hauser, Longo, et al. (2008) HARRISON'S INTERNAL MEDICINE(Disorders of the Kidney & Urinary Tract) 17.
- Pratsinis A, Devuyst O, Leroux JC (2013) Peritoneal dialysis: use beyond terminal chronic renal failure 282:3-12
- Banaga AS, Mohammed EB, Siddig RM, Salama DE, Elbashir SB, et al. (2015) Causes of end stage renal failure among haemodialysis patients in Khartoum State/Sudan. BMC Research Notes 8:502.
- Ma TK, Chow KM, Kwan BC, Ng JK, Pang WF, et al. (2017) The choice of comorbidity scoring system in Chinese peritoneal dialysis patients. Clinical and experimental nephrology 22: 159-166.
- Jablonski A (2007) The multidimensional characteristics of symptoms reported by patient on hemodialysis. Nephrol Nurse Journal 34: 29-38.
- Lee ET, Go OT (1997) Survival Analysis in Public Health Research. Public Health 18: 105-34.
- Khairi S, Faghihzadeh S, Meshkani M, Mahmoudi M, babaei G (2003) Comparison of Stimates Parameters in Cox and Frailty Models with Unknown Risk Factors. Research in Medical Sciences 8: 2.
- Leung KM, Elashoff RM, Afifi AA (1997) Censoring issues in survival analysis. Annu Rew Public Health 18: 83-104.
- Keiding N, Andersen PK, Klein P (1997) The role of frailty models and accelerated failare time models in describing heterogeneity due to omitted covariates. Statistics in Medicine 16: 215-224.
- Hougaard P (2000) Analysis of multivariate survival data. New York: Springer-Verlag 2000. International J of Epidemiol 30:909-910.
- Wienke A (2007) Frailty Models in Survival Analysis.University Halle-Wittenberg.Germany: ULB-Sachsen-Anhalt.
- Clayton D (1991) A monte carlo method for Bayesian inference in frailty modelsBiometrics 47: 467-85.
- Hougaard P (1997) Frailty: In Encyclopedia of Biostatistics. Armitage P, Colton T, editors. New York: Wiley.
- Klein JP, Moeschberger ML (2003) Survival analysis : techniques for censored and truncated data. Springer-Verlag.
- Kutner MH, Nachtsheim JC, Neter J, Li W (2005) Applied Linear Statistical Models. Mc Graw Hill Companies.
- Haghighi F, Nikulin M (2007) A Chi-Square test for Power Generalized Weibull Family for the Head-and-Neck cancer censored data. Journal of Mathematical Sciences 133:1333-1352.
- Kleinbaum DG, Klein M (2005) Survival Analysis-A Self-Learning Text. Second ed. United States of America: Springer 294-295
- Duchateau L, Janssen P (2008) Statistics for Biology and Health-The Frailty Model. USA Springer 32-36.
- Smeltzer S, Bare B, Hinkle J, Cheever K (2010) Brunner and Suddarth's Textbook of Medical-Surgical Nursing, Lippincott Williams & Wilkins 9: 1328.
- Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J (2008) Harrison's Principles of Internal Medicine, Kidney and Urinary Tract Disorders. Samat 130-136.
- SaCarvalho M, Henderson R, Shimakura S (2003) Survival of hemodialysis patients: modeling differences in risk of dialysis centers. International Journal for Quality in Health Care 15:189-196.
- Ghadimi M, Mahmoudi M, Mohammad K, Hosseini M, Rasouli M (2011) Factors Affecting Survival of Patients with Gastric Cancer Using Frailty Models. Journal Payesh 10: 522-53.
- Ponnuraja C, Venkatesan P (2010) Correlated Frailty Model: An Advantageous Approach For Covariate Analysis Of Tuberculosis Data. Indian Journal of Science and Technology 3: 151-155.
- Argyropoulos C, Chang C-C, Planting L, Fink N, Powe N, (2009) Considerations in the Statistical Analysis of Hemodialysis Patient Survival. Journal of American Society of Nephrology 20: 2034-2043.
- Yeates A, Hawley C, Mundy J, Pinto N, Haluska B, et al. (2012) Treatment outcomes for ischemic heart disease in dialysis- dependent patients. Asian Cardiovascular & Thoracic Annals 20: 281-291.
- Ahuja ST, Grady J, Khan S (2002) Changing Trends in the Survival of Dialysis Patients with Human Immunodeficiency Virus in the United States. Journal of American Society of Nephrology 13: 1889-1893.
- Lin H-H, Tsai C-W, Lin P-H, Cheng K-F, Wu H-D, et al. (2012) Survival analysis of pediatric dialysis patients in Taiwan. NEPHROLOGY 17: 621-627.
- Montaseri M, Charati JY, Espahbodi F (2016) Application of Parametric Models to a Survival Analysis of Hemodialysis Patients. Nephrourol Mon 8: e28738.
- Montaseri M, Yazdani Cherat J, Espahbodi F, Mousavi SJ (2013) Five-year Survival Rate in Hemodialysis Patients Attending Sari Imam Khomeini Hospital. Journal of Mazandaran University of Medical Sciences 23: 78-85.
- Jungers P, Massy AZ, Nguyen-Khoa T, Choukroun G, Robino C, et al. (2001) Longer Duration of Predialysis Nephrological Care is Associated with improved Long-Term Survival of Dialysis Patients. Nephrology Dialysis Transplantation 16: 2357-2364.
- Herzog CA, Ma JZ, Collins AJ (2002) Comparative Survival of Dialysis Patients in the United States After Coronary Angioplasty, Coronary Artery Stenting, and Coronary Artery Bypass Surgery and Impact of Diabetes. Journal of the American Heart Association 106: 2207-2211.
- khavaninzadeh M, Omrani Z, shirAli A, Najmi N, Mommadzadeh M, et al. (2007) Determination of Prevalence and Survival of Various Types of Vascular Accesses in Patients With End Stage Renal Disease Under Chronic Hemodialysis, in Tehran during 2004. Journal of Iran Medical University 15: 71-76.
- Traynor Jp, Simpson K, Geddes CC, Deighan CJ, Fox GJ (2002) Early Initiation of Dialysis Fails to Prolong Survival in Patients with End-Stage Renal Failure. Journal of the American Society Nephrology 13: 2125-2132.
- Feng L, Jin AZ, Allen JC, Chow KY, Jafar TH (2017) Timing of commencement of maintenance dialysis and mortality in young and older adults in Singapore. BMC Nephrology18: 176.
- Mousavi SB, Nejad KH, Zeraati A (2010) The Evaluvation of Dialysis Adequacy by KT/V in Hemodialysis Patients.
- Liu K, Himmelfarb J, Paganini E, Ikizler T, Soroko S, et al. (2006) Timing of initiation of dialysis in critically ill patients with acute kidney injury. Clin J Am Soc Nephrol 1: 915-9.
- Namdar A, Beigizadeh S, Najafipour S (2013) Health- related quality of life in dialysis patients. J of Jahrom University of Medical Sciences10: 19-27.
- Jhamb M, McNulty ML, Ingalsbe G, Childers JW, Schell J,et al. (2016) Knowledge, barriers and facilitators of exercise in dialysis patients: a qualitative study of patients, staff and nephrologists. BMC Nephrology 17.
- Johansen K, Chertow G, Jin C, Kutner N (2007) Significance of Frailty among Dialysis Patients. J Am Soc Nephrol 18:2960-2967.
Citation: Montaseri M, Dindarloo MM, Fatemeh Espahbodi F and Charati YN (2023) Factors Influencing Hemodialysis Patients Survival Using Frailty Models. J Nephrol Renal Ther 9: 083.
Copyright: © 2023 Maryam Montaseri, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.