Megaprosthesis Revision Caused by Aseptic Loosening and Nonunion of the Structural Allograft in Patients Younger Than 40 Years
*Corresponding Author(s):
Luis Gerardo Natera CisnerosDepartment Of Orthopaedics And Traumatology, Hospital General De Catalunya, Street Pedro I Pons 1, Sant Cugat Del Vallés, Barcelona 08190, Spain
Tel:+34 600393826,
Email:luisgerardonaterac@gmail.com
Abstract
Background: The use of structural allografts is aimed to restore the resected bone segment in order to maintain enough bone stock for future revisions. The aim of this study was to describe the mechanical failures of Allograft Megaprosthesis Composite (AMC) revised to Modular Megaprosthesis (MMP) due to nonunion of the structural allograft in patients younger than 40 years.
Material and methods: A retrospective revision in a referral hospital for the treatment of musculoskeletal tumors was performed between January 1st 2009 and January 31st 2012. We looked in the surgical records of the musculoskeletal tumors unit for all of the procedures coded as “megaprosthesis-revision-arthroplasty”. We included patients younger than 40 year-old in which primary reconstructive surgery at any segment of the lower limb was performed by means of AMC, and revision surgery was performed by means of MMP. We looked in those records for information regarding integration of the structural allograft to the native bone.
Six revisions from AMC to MMP were performed: 5 knees and 1 hip. The mean age at the time of revision surgery was 28.83 year-old (range 18-38). Primary oncological diagnoses were: 4 osteosarcomas of the distal femur, one Giant Cell Tumor (GCT) of the femoral head and 1 GCT of the proximal tibia.
Results: In none of the cases integration of the structural bone allograft to the native bone was observed, reason why it had to be completely resected in all patients. The reason for revision surgery in all cases was aseptic loosening secondary to nonunion of the structural bone allograft. Mean time elapsed from implantation of AMC to revision surgery to MMP was 103 months. Mean time elapsed from revision surgery to last follow-up visit was 26 months.
Conclusion: Structural bone allografts in limb salvage surgery after massive tumor resection, may not be the best reconstructive option because the high probability that the grafted bone segment might not integrate to the native bone, even in young patients, may lead to prosthetic failure because of aseptic loosening.
Keywords
LEVEL OF EVIDENCE:
INTRODUCTION
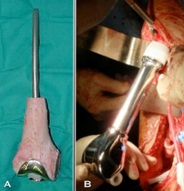
Figure 1: Allograft prosthesis composite before being implanted (A), distal femur modular megaprosthesis once implanted (B).
The published overall megaprosthesis survival is 57-93% at 5 years [8] and 50-88% at 10 years [9]. These implants are usually employed in young patients with high functional demands and a bone quality affected by concomitant radio and chemotherapy, reasons that might suppose a high risk for failure [8]. Infections represent the main reason for revision surgery of these implants, and this issue is mainly due to the immunosuppression secondary to the adjuvant therapies [10].
The development of the prosthetic implants and components modularity have supposed an increase in the use of MMP and a decrease in the use of AMC, because MMP suppose a shorter surgical time and intraoperative availability of several modules that allow adaptations when there is to change the planned resection. Likewise, the post-operative period of a MMP does not require long times of non-weight bearing that, in cases of AMC, are indicated in order to protect the integration of the allograft to the host-bone, reason why MMP allow a faster return to function [11,12].
According to some authors, the use of structural allografts in AMC is aimed to restore the resected bone segment, to offer a bed in which musculotendinous structures can be reinserted, and to guarantee enough bone stock for future revisions once integrated to the host-bone [13].
The aim of this study was to describe the mechanical failures of AMC revised to MMP due to nonunion of the structural allograft in patients younger than 40 years at the moment of revision surgery. The secondary aim was to estimate the mean survival of the primary implant (AMC).
MATERIAL AND METHODS
The total number of cases that met the inclusion criteria was 6: 5 knees and 1 hip (Figures 2-5). The mean age of the included patients at the time of revision surgery was 28.83 year-old (range 18-38). The primary oncological diagnoses were: 4 osteosarcomas of the distal femur, 1 Giant Cell Tumor (GCT) of the femoral head and 1 GCT of the proximal tibia. In all of the primary implants (AMC) structural bone allograft was used. There were 3 men and 3 women. The primary AMC in all cases was a custom made implant Waldemar-link (Hamburg, Germany). 4 of the AMC were cemented and 2 were not. The surgical approaches employed at the primary surgery were: a midline extended approach to the knee joint in cases 1-4 and 6; and an extended posterolateral approach to the hip joint in case number 5. Frozen structural allografts were used in all cases. Revision surgery was performed through the surgical scar of the previous approach in all cases. The revision MMP used in all cases was Waldemar-link, all of them cemented. All of these procedures involved a high complexity, and were all performed by the senior surgeon IG. All of the patients had surgery under general anesthesia and femoral nerve block. In all patients antibiotics were administrated intraoperatively and during the whole period of hospitalization, according to the protocol established in our institution. 2g of cefazolin were administrated during surgery once tissue samples for microbiology examination were taken. 1g of cefazolin was administrated every 8h until discharge. Low-molecular heparin prophylaxis was given from the day of admission until 30 days after discharge. All of the patients had surgery without tourniquet in order to have a better control of the neurovascular bundle.

Figure 2: Aseptic loosening and nonunion of the structural allograft in an allograft megaprosthesis composite. The lysis of the allograft caused a shortening of the femur and extrusion of the stem through the great trochanter (A); distal femur modular megaprosthesis as revision mega-arthroplasty (B).



RESULTS
Radiographic follow-up
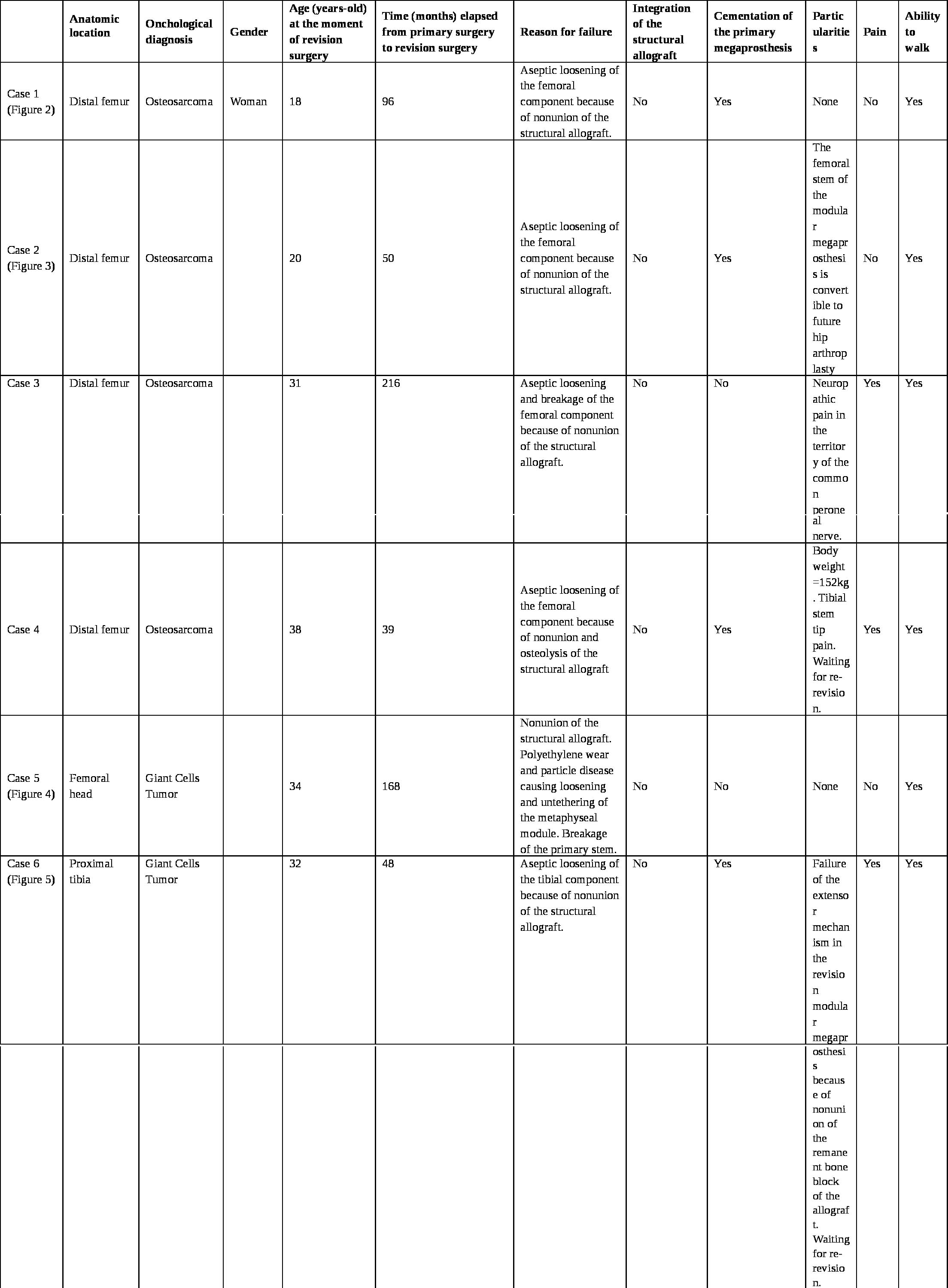
Table 1: Details of the 6 cases of patients with failed custom-made allograft prosthesis composite because of nonunion of the structural allograft and aseptic loosening.
Clinical follow-up evaluations
Complications related to revision surgery
DISCUSSION
Megaprosthesis are big constrained implants with long lever arms that confer a high stress at the interface “implant-cement-bone”, reason why they can be considered with propensity to eventual mechanical failure [15]. Regarding the reasons for failure of these implants, a retrospective multicentric revision published by Henderson et al., in 2011 describe 5 types of failure [16]. They describe that aseptic loosening is the second reason for failure in terms of frequency, and infection is the main one. According to this classification, all of the AMC of our series belongs to the type II (aseptic loosening).
Aseptic loosening is considered as the final consequence of a series of mechanical factors common to all the megaprosthesis. It has been attributed to: a long interface “implant-cement-bone” [17], to the stresses generated by the important lever arms of the constrained hinges [15], by an altered transmission of the axial loads when walking [7], and high functional demands of young patients [18]. Besides these reasons, we believe that the fact that the structural allograft did not integrate in any of the cases of our series had a determinant role in the development of the aseptic loosening and the subsequent failure of the megaprosthesis.
In our series the mean age of the patients at the time of revision surgery was 29 year-old, while in other published series of megaprosthesis revision surgery, the mean age of patients at the moment of implantation of the primary megaprosthesis was 41 [16] and 27 year-old [19]. Despite our series have a low number of cases, it is confirmed by patients in which revision surgery was performed with a mean age lower than the mean age at the moment of the primary surgery of other published series. We believe that the fact that the structural allograft had to be removed in all of the cases of our series (despite the theoretical biological advantages of the young patient in terms of bone consolidation and integration, and despite the five-year survival of massive allograft reconstructions has been described to be 80.8% [20]) denotes that the reconstructive strategy with AMC could be at least questionable.
One of the theoretical advantages of an AMC in those cases of resection of the proximal tibia, is that the structural allograft allows a reinsertion of the extensor mechanism when the resection compromises the Anterior Tibial Tuberosity (ATT). Donati et al., reported a survival of 78% at five years in cases of resection of the proximal tibia managed with AMC as a primary Surgery [21], reporting that 12.9% of their patients underwent additional surgery to promote union of the graft. They also describe that union of the graft could be negatively conditioned by the use of radiotherapy. Our experience has led us to believe that in this kind of patients, structural allografts behave as a temporary spacer, so union to the native bone is something that rarely occurs. In case number 6 of our series, the proximal segment of the tibia had to be completely resected at the moment of revision surgery, but a bone block with the ATT could be preserved. The primary reconstruction strategy consisted in an AMC in order pretend integration of the bone block with the ATT to the structural allograft. In this case, neither the structural allograft integrated to the host-bone nor the ATT integrated to the structural allograft.
In regards to the mechanical failures and the mean survival of the AMC and the MMP, Biau et al., described in their series of 91 megaprosthesis that mechanical failures were more frequent in AMC (10/33) than in MMP (10/58), and that the mean survival of AMC was 117 months and of MMP 138 months [19]. In another series of 75 knee megaprosthesis, Wunder et al., described that the failure proportion was greater in the group of AMC when compared to the group of MMP (6/10 vs 10/64 respectively) [22]. It could be considered that nowadays there is enough evidence to establish that a MMP is a superior reconstruction strategy than an AMC. Based on the mentioned premises, actually in our unit all of the primary and revision megaprosthesis are MMP.
Our study has the limitation of being a retrospective revision with a low number of cases, with a heterogeneous pathology and with several anatomic locations. However, our revision has the strength of being conformed by a series of young patients in which all of them had a revision of the megaprosthesis only because of mechanical failures, when they were younger than 40 year-old.
The results of our revision allow us to conclude that the use of structural allografts in limb salvage surgery after massive tumor resection, may not be the best reconstructive option because the high probability that the grafted bone segment might not integrate to the native bone, even in young patients, may lead to prosthetic failure because of aseptic loosening.
The study was performed in accordance with the ethical standards of the Declaration of Helsinki (amended in October 2013); and the level of confidentiality concerning the protection of personal data was as required by the Spanish laws (LOPD 15/1999). All patients gave their written informed consent, and they accepted that data from their electronic medical file could be used for purposes of this scientific research.
REFERENCES
- Rougraff BT, Simon MA, Kneisl JS, Greenberg DB, Mankin HJ (1994) Limb salvage compared with amputation for osteosarcoma of the distal end of the femur. A long-term oncological, functional, and quality-of-life study. J Bone Joint Surg Am 76: 649-656.
- Gross AE, McKee NH, Pritzker KP, Langer F (1983) Reconstruction of skeletal deficits at the knee. A comprehensive osteochondral transplant program. Clin Orthop Relat Res 96-106.
- Enneking WF, Eady JL, Burchardt H (1980) Autogenous cortical bone grafts in the reconstruction of segmental skeletal defects. J Bone Joint Surg Am 62: 1039-1058.
- Harris AI, Gitelis S, Sheinkop MB, Rosenberg AG, Piasecki P (1994) Allograft prosthetic composite reconstruction for limb salvage and severe deficiency of bone at the knee or hip. Semin Arthroplasty 5: 85-94.
- Capanna R, Morris HG, Campanacci D, Del Ben M, Campanacci M (1994) Modular uncemented prosthetic reconstruction after resection of tumours of the distal femur. J Bone Joint Surg Br 76: 178-186.
- Malawer MM, Chou LB (1995) Prosthetic survival and clinical results with use of large-segment replacements in the treatment of high-grade bone sarcomas. J Bone Joint Surg Am 77: 1154-1165.
- Plötz W, Rechl H, Burgkart R, Messmer C, Schelter R, et al. (2002) Limb salvage with tumor endoprostheses for malignant tumors of the knee. Clin Orthop Relat Res 207-215.
- Wirganowicz PZ, Eckardt JJ, Dorey FJ, Eilber FR, Kabo JM (1999) Etiology and results of tumor endoprosthesis revision surgery in 64 patients. Clin Orthop Relat Res 64-74.
- Asavamongkolkul A, Eckardt JJ, Eilber FR, Dorey FJ, Ward WG, et al. (1999) Endoprosthetic reconstruction for malignant upper extremity tumors. Clin Orthop Relat Res 207-220.
- Berbari EF, Hanssen AD, Duffy MC, Steckelberg JM, Ilstrup DM, et al. (1998) Risk factors for prosthetic joint infection: case-control study. Clin Infect Dis 27: 1247-1254.
- Guo W, Ji T, Yang R, Tang X, Yang Y (2008) Endoprosthetic replacement for primary tumours around the knee: experience from Peking University. J Bone Joint Surg Br 90: 1084-1089.
- Zeegen EN, Aponte-Tinao LA, Hornicek FJ, Gebhardt MC, Mankin HJ (2004) Survivorship analysis of 141 modular metallic endoprostheses at early followup. Clin Orthop Relat Res 239-250.
- Raskin KA, Hornicek F (2009) Allograft reconstruction in malignant bone tumors: indications and limits. Recent Results Cancer Res 179: 51-58.
- Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ (1993) A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res 241-246.
- Taylor SJ, Walker PS, Perry JS, Cannon SR, Woledge R (1998) The forces in the distal femur and the knee during walking and other activities measured by telemetry. J Arthroplasty 13: 428-437.
- Henderson ER, Groundland JS, Pala E, Dennis JA, Wooten R, et al. (2011) Failure mode classification for tumor endoprostheses: retrospective review of five institutions and a literature review. J Bone Joint Surg Am 93: 418-429.
- Jeon DG, Kawai A, Boland P, Healey JH (1999) Algorithm for the surgical treatment of malignant lesions of the proximal tibia. Clin Orthop Relat Res 15-26.
- Mittermayer F, Krepler P, Dominkus M, Schwameis E, Sluga M, et al. (2001) Long-term followup of uncemented tumor endoprostheses for the lower extremity. Clin Orthop Relat Res 167-177.
- Biau D, Faure F, Katsahian S, Jeanrot C, Tomeno B, et al. (2006) Survival of total knee replacement with a megaprosthesis after bone tumor resection. J Bone Joint Surg Am 88: 1285-1293.
- Bullens PH, Minderhoud NM, de Waal Malefijt MC, Veth RP, Buma P, et al. (2009) Survival of massive allografts in segmental oncological bone defect reconstructions. Int Orthop 33: 757-760.
- Donati D, Colangeli M, Colangeli S, Di Bella C, Mercuri M (2008) Allograft-prosthetic composite in the proximal tibia after bone tumor resection. Clin Orthop Relat Res 466: 459-465.
- Wunder JS, Leitch K, Griffin AM, Davis AM, Bell RS (2001) Comparison of two methods of reconstruction for primary malignant tumors at the knee: a sequential cohort study. J Surg Oncol 77: 89-99.
Citation: Cisneros LGN, Trullols L, Moya E, Peiró A, Gracia I (2015) Megaprosthesis Revision Caused by Aseptic Loosening and Nonunion of the Structural Allograft in Patients Younger Than 40 Years. J Orthop Res Physiother 1: 016.
Copyright: © 2015 Luis Gerardo Natera Cisneros, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.