Obstructive shock as presentation of an abdominal mass - Case Report
*Corresponding Author(s):
Joana VilaçaPediatric Department, Hospital De Braga, Braga, Portugal
Tel:+351 916566764,
Email:joana.gvilaca@gmail.com
Sofia Brandão Miranda
Pediatric Department, Hospital De Braga, Braga, Portugal
Tel:+351 926702396,
Email:asofiabmiranda@gmail.com
Abstract
Introduction
Obstructive shock is the least common type of pediatric shock. It results from obstruction of cardiac output, with intra-abdominal masses being a rare cause.
Description of the case
We report a case of a healthy 2-month-old infant who developed obstructive shock secondary to compression of the abdominal aorta, resulting in impairment of cardiac function due to an abdominal mass.
Discussion
Wilms tumor represents 7% of neoplasms in infants. The most common presentation is an abdominal mass, and it is extremely rare to present with obstructive shock. In this case, the age and form of presentation were atypical, but recognition and rapid medical and surgical intervention allowed for clinical stabilization and recovery of cardiac function. This case highlights the importance of recognition and proper management in cases of obstructive shock. Although rare, abdominal masses should be considered in the differential diagnosis
Keywords
Abdominal mass; Emergent surgery; Infant; Obstructive shock; Wilms tumor
Key-messages
Obstructive shock is the least common type of pediatric shock.
Wilms tumor is the second most common pediatric intra-abdominal tumor.
This case demonstrates a rare presentation (obstructive shock) of one of the most common pediatric intra-abdominal tumors.
Introduction
Shock is a life-threatening condition caused by the systemic failure of the circulatory system. Obstructive shock is the least common cause of shock in pediatrics [1], and an abdominal mass is a rare cause of this type of shock. Only a few reported cases of pediatric Wilms tumor have presented during the first months of life, and none have presented with obstructive shock [2]. Our case is interesting and challenging, as it features obstructive shock due to an abdominal mass that was later diagnosed as a Wilms tumor.
Description Of The Case
A healthy 2-month-old infant boy with regular follow-up, no relevant prenatal, neonatal, or familial history, was taken to the Emergency Department of a secondary hospital due to respiratory distress, groaning, and food refusal within one day of evolution. On physical examination, he was apyretic, with marbled skin, tachypnea, tachycardia, hypotension, and marked abdominal distension with palpation of a hard abdominal mass throughout the left abdomen extending beyond the abdominal midline. It was decided to start sedoanalgesia and intubation. Hemodynamic improvement was observed after volume expansion with two boluses. Analytically, there was metabolic acidosis (pH 7.234, pCO2 39.9 mmHg, HCO3- 16.9 mmol/L) and hyperlactacidemia (9.3 mmol/L), LDH 788 U/L and D-dimers 2570 ng/mL. Thoraco-abdomino-pelvic tomography revealed a bulky abdominal mass (8.5 x 9 x 10 cm) without calcifications, poor individualization of the left kidney and adrenal gland on the same side. This mass extends medially, becoming inseparable from the retroperitoneal structures, including the great vessels, and inferiorly extends to the left iliac fossa (Figure 1). He was transferred to the Pediatric Intensive Care Unit (PICU).
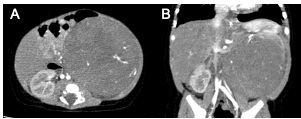 Figure 1: Non-contrast abdominal CT; A - Axial cut showing a large abdominal mass on the left with soft tissue density, measuring 8.5x9 cm in maximum axial diameters, extending medially and becoming inseparable from retroperitoneal structures, including large vessels; B- Coronal cut showing the mass extending to the left iliac fossa, measuring 10cm in length."
Figure 1: Non-contrast abdominal CT; A - Axial cut showing a large abdominal mass on the left with soft tissue density, measuring 8.5x9 cm in maximum axial diameters, extending medially and becoming inseparable from retroperitoneal structures, including large vessels; B- Coronal cut showing the mass extending to the left iliac fossa, measuring 10cm in length."
On admission in the PICU, he had cold extremities, tachycardia, P5 blood pressure, grade II/VI murmur, and filiform pedal and femoral pulses. The echocardiogram showed left chamber dilatation, left ventricular dysfunction, left ventricular ejection fraction (LVEF) 30%, and fractional shortening (Fenc) 19%, mild mitral, tricuspid, and aortic regurgitation. Due to obstructive shock due to compression of abdominal aorta for the abdominal mass, an exploratory laparotomy was decided with excision of the abdominal mass, and left nephrectomy (after obtaining parents’ consent). Intraoperative findings demonstrated a left retroperitoneal mass attached to the left kidney. After surgical removal, the mass was sent for histopathological evaluation. Less than twenty-four hours after the surgery, an echocardiogram showed improvement in cardiac function with LVEF 50% and Fenc 25%, hemodynamically stable without aminergic support. He was extubated the day after the surgery.
The histological exam revealed a Wilms Tumor (TW) and the infant was transferred to the oncology pediatric center. He completed a cycle of chemotherapy with vincristine, without complications. Currently, about 6 months after diagnosis, the infant is asymptomatic and has slight dilation of the left ventricle, LVEF 55% and Fenc 28%. He maintains clinical and imaging surveillance at a pediatric oncology center, with no significant problems.
Discussion
Wilms tumor, also known as nephroblastoma [2], is the most common primary renal [1] tumor in children, accounting for 95% of all renal malignancies in children [3]. It is the fourth most common pediatric cancer overall [4]. After neuroblastoma, it is the second most common pediatric intra-abdominal tumor, accounting for 6% of overall childhood malignancies. About 95% of cases of Wilms tumors are sporadic, and in some cases may occur in association with other congenital malformations. The average age at diagnosis of Wilms tumor is 4 years, with most cases appearing between ages 2 and 5 years. In patients with unilateral involvement, the median age at diagnosis is 43 months in girls and 37 months in boys[1].
Most children with Wilms tumor present with an abdominal mass or swelling, without other signs or symptoms. A silent abdominal mass, typically brought to medical attention by the caregiver while bathing the child or changing clothes, is the most common mode of presentation [1].
Common differential diagnoses of abdominal masses include tumors such as neuroblastoma, Wilms tumor, rhabdoid tumor, mesoblastic nephroma, and clear cell sarcoma. Other causes include polycystic kidney disease and pyelonephritis [6].
Obstructive shock as a presentation of Wilms tumor is extremely rare. To the best of our knowledge, we were unable to find any documented cases in the published literature. Presentation at this age is also unusual. Despite regular follow-up and no previously described abdominal mass, a prenatal tumor may be considered. Obstructive shock is a less common, but important cause of shock in critically ill infants and children. The most common causes generally include tension [7] pneumothorax, cardiac tamponade, and pulmonary embolism [8]. Also included in this category physiologically, and more specific to pediatrics, are congenital heart lesions characterized by left ventricular outflow tract obstruction, including critical aortic stenosis, coarctation of the aorta, interrupted aortic arch, and hypoplastic left heart syndrome [7]. In this case, we report an abdominal tumor as the cause of this shock. Compression of the abdominal aorta caused obstruction of the left ventricular outflow tract. Despite the research carried out by the authors, no report of an abdominal mass causing obstructive shock in pediatric age was found.
In conclusion, we present a case of a rare presentation of Wilms Tumor (abdominal mass causing obstructive shock) in an unusual age.
References
- Green M (2021) Paediatric Shock. TeachMe Paediatrics.
- Ahmed S, Nadarajan C, Ng Chiak Yot, Teh YG, Abdul Muien MZ, et al. (2021) Wilms tumor presenting as small bowel obstruction in a neonate: A diagnostic challenge. Radiol Case Rep 16: 2908-2912.
- Kajal K, Munirathinam GK, Mandal B, Gandhi K, Singh H, et al. (2018) Wilm's tumor with intracardiac extension causing dynamic tricuspid valve obstruction: An anesthetic challenge. Case report. Saudi J Anesthesia 12: 321-323.
- Leslie SW, Sajjad H, Murphy PB (2022) Wilms Tumor. In: StatPearls.
- Smith V ,Chintagumpala M (2022) Presentation, diagnosis, and staging of Wilms tumor.
- Chung EM, Graeber AR, Conran RM (2016) Renal Tumors of Childhood: Radiologic-Pathologic Correlation Part 1 The 1st Decade From the Radiologic Pathology Archives. RadioGraphics 36: 499-522.
- Morgan C, Wheeler DS (2013) Obstructive Shock. The Open Pediatric Medicine Journal 7: 35-37.
- Margaretha PA, Rusmawatiningtyas D, Makrufardi F, Kumara IF, Nurnaningsih (2021) Obstructive shock in pediatric patient with congenital cystic adenomatoid malformation: A case report. Ann Med Surg Lond.
Citation: Vilaça J, Miranda SB, Nogueira MV, Henriques C, Fernandes SR, et al. (2023) Obstructive shock as presentation of an abdominal mass - Case Report. J Neonatol Clin Pediatr 10: 104.
Copyright: © 2023 Joana Vilaça, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.