Plantar Inserts Therapy for Hind Foot Subtalar Joint Valgus Type in Medial Gonarthrosis
*Corresponding Author(s):
Shingo ShimizuFaculty Of Health, Medical And Welfare, Saitama Prefecural University, Japan
Tel:+81 489734123,
Email:shimizu-shingo@spu.ac.jp
Abstract
Here are two types of knee osteoarthritis: one type in which the subtalar joint is varus and the other type in which the subtalar joint is Valgus.
Although there have been previous studies on the effectiveness of plantar inserts for the subtalar joint varus type, there have been no studies regarding the effectiveness of plantar inserts for the subtalar joint valgus type.
In this study, a subtalar joint valgus-inducing plantar insert and a subtalar joint varus-inducing plantar insert were installed and compared for patients with subtalar joint valgus type of knee osteoarthritis.
The subjects were 40 knees of 20 patients who were diagnosed with medial type knee osteoarthritis, had no restriction in knee extension, and had both subtalar joints valgus as observed by walking and footprints.
The methods are maximum effort 10m walking time, maximum effort 10m walking pain, TUG clockwise time and pain, counterclockwise time and pain, and FRT.
As a result, the varus-guided plantar insert showed the most significant improvement in the subtalar joint valgus type.
In addition, in one case, the long-term effectiveness of varus-guided plantar inserts for subtalar joint valgus type showed improvements in pain, number of steps, energy expenditure, body weight, body fat percentage, etc.
Plantar inserts for knee osteoarthritis do not simply prescribe subtalar joint valgus-guided using a lateral wedge, but instead perform individual evaluations and provide plantar inserts for subtalar joint neutral-guided to improve individual alignment.
Keywords
Knee osteoarthritis; Plantar plate effectiveness; Neutral; Subtalar joint
Introduction
Medial knee osteoarthritis includes subtalar joint varus type and subtalar joint valgus type, and guidance of the subtalar joint is important when performing plantar inserts therapy [1].
For subtalar joint varus type and subtalar joint valgus type, subtalar joint valgus-guiding plantar insert using a lateral wedge is said to be effective [2,3].
On the other hand, there are also reports that subtalar joint varus-guided plantar inserts are good for subtalar joint valgus types [4,5].
Furthermore, there are currently no reports on the use of subtalar joint varus-inducing plantar inserts for subtalar joint valgus types.
Therefore, in this study, we attached two types of plantar inserts, a subtalar joint valgus-inducing plantar insert and a subtalar joint varus-inducing plantar insert, to patients with subtalar joint valgus type of knee osteoarthritis. By comparing these results, we investigated plantar inserts for the subtalar joint valgus type.
Furthermore, we investigated the long-term effectiveness of subtalar joint varus-guided plantar inserts in one patient with bilateral subtalar joint valgus type.
Subject
The subjects were 40 knees of 20 patients who had been diagnosed with medial type knee osteoarthritis, had no restriction in knee extension, and had both subtalar joints in valgus when observed by walking and footprints.
Subjects had an average age of 65 ± 6 years, an average height of 155 ± 7 cm, an average weight of 56 ± 8 kg, an average Femorotibial Angle (FTA) of 179 ± 3 degrees, an Kellgren-Lawrence (KL) classification of 15 knees in I and 11 knees in II. There were 13 knees with III and 1 knee with IV.
How To Make Plantar Inserts
It was manufactured using two types of pads: a pad manufactured by EMSOLD in Germany and a Sorbo pad manufactured by Sanshin Kosan.
The subtalar joint valgus guiding plantar insert is attached to the medial arch using the DSIS 3-axis arch pad® and DSIS R wedge pad® so as not to touch the talus process of the calcaneus behind the medial arch, and the subtalar joint is lateralized. It was made to guide the robot in the opposite direction (Figure 1).
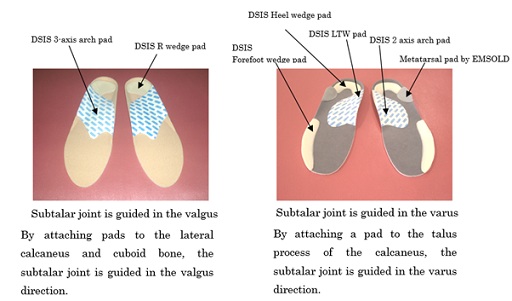 Figure 1: Plantar insert.
Figure 1: Plantar insert.
The subtalar joint varus guiding plantar insert is attached to the using the DSIS 2-axis arch pad®, DSIS LTW Pad®, DSIS Heel Wedge Pad®, and Metatarsal Pad® manufactured by EMSOLD in Germany are used to attach the medial arch to the posterior calcaneus talus process. The subtalar joint was affixed so as to extend in the direction of varus, and was made to guide the subtalar joint in the varus direction [6] (Figure 1).
In addition, for the subtalar joint varus-inducing plantar insert, a DSIS forefoot wedge pad® was attached to the anterolateral side to induce kicking to the big toe during late stance [6] (Figure 1).
Methods
In a previous study by Okubo et al., a normal hindfoot was defined as within ±2 degrees from 0 degrees perpendicular to the floor surface, and subtalar joint valgus was defined as a hindfoot inclination of 3 degrees or more inward [7] (Figure 2).
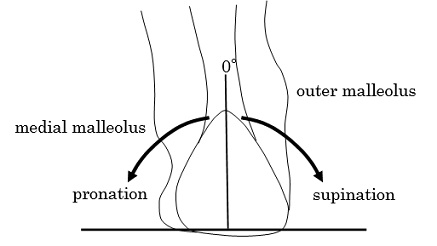 Figure 2: Evaluation of the subtalar joint.
Figure 2: Evaluation of the subtalar joint.
Normal within 2° based on 0°, Varus and valgus at 3° or more
The order of attachment of the subtalar joint valgus-guiding plantar insert, subtalar joint varus-guiding plantar insert, and non-applying the plantar insert were changed after each measurement in each case, taking into consideration the learning effect. Measurements were made three times with different values and the average values were compared.
The evaluation items were maximum effort 10m walking time, pain during maximum effort 10m walking, Time Up Go Test (TUG) clockwise time and pain, counterclockwise time and pain, and Functional Reach Test (FRT).
Pain was evaluated using a 100 mm line segment on a visual analogue scale (VAS), with the most painful time being 100 mm and no pain being 0 mm. The statistical software used was J-STAT, and the Wilcoxon signed rank sum test was used to set the significance level to less than 5%.
Results
The 10m walking time was significantly improved with the subtalar joint valgus-inducing plantar insert and the subtalar joint varus-inducing plantar insert compared to not wearing it. There was no significant difference between subtalar joint valgus-guided plantar inserts and subtalar joint varus-guided plantar inserts. Pain when walking 10 m was significantly improved with the subtalar joint valgus-inducing plantar insert and the subtalar joint varus-guiding plantar insert compared with not wearing it, and the subtalar joint varus-inducing plantar insert was significantly better than with the subtalar joint valgus-inducing plantar insert (Table 1).
|
|
Not installed |
Valgus-induction |
Varus-induction |
|
10m walking time (s) |
8.5±1.4 |
7.9±1.3** |
7.8±1.3** |
|
Pain when walking 10m(mm) |
25.0±18.0 |
19.0±19.0** |
9.0±14.0**## |
|
TUG clockwise time (s) |
8.0±1.5 |
7.8±1.5* |
7.4±1.5**## |
|
TUG pain turning clockwise (mm) |
31.0±17.0 |
26.8±15.2** |
15.8±11.4**## |
|
TUG counterclockwise time (s) |
7.9±1.5 |
7.8±1.5 |
7.5±1.3*# |
|
TUG pain turning clockwise (mm) |
32.5±16.1 |
24.9±13.8** |
16.8±12.3**## |
|
FRT(mm) |
277±28 |
280±36 |
309±31**## |
Table 1: Comparison of hindfoot pronation type with plantar insert attached.
Comparison with non-wearing *:p < 0.05 **: p < 0.01
Comparison of valgus induction and varus induction #:p < 0.05 ##p< 0.01
n(10m walking time, TUG time, FRT) = 20
n(Pain when walking 10m, pain when TUG) = 40
When turning clockwise of the TUG significantly improved the subtalar joint valgus-inducing plantar insert and the subtalar joint varus-inducing plantar insert than when not wearing it, and the subtalar joint varus-inducing plantar insert was significantly better than with the subtalar joint valgus-inducing plantar insert (Table 1).
When turning the TUG counterclockwise, there was no significant difference between the when not wearing and the subtalar joint valgus-inducing plantar inserts, but there was a significant improvement in the subtalar joint varus-inducing plantar inserts compared to the non-wearing TUG. In addition, subtalar joint varus-guided plantar inserts were significantly improved compared to subtalar joint valgus-guided plantar inserts (Table 1).
TUG pain was significantly improved with subtalar joint valgus-inducing plantar inserts and subtalar joint varus-inducing plantar inserts compared with non-wearing, and the subtalar joint varus-inducing plantar insert was significantly better than with the subtalar joint valgus-inducing plantar insert (Table 1).
FRT was no significant difference between the when not wearing and the subtalar joint valgus-inducing plantar inserts, but there was a significant improvement in the subtalar joint varus-inducing plantar inserts compared to the non-wearing. In addition, subtalar joint varus-guided plantar inserts were significantly improved compared to subtalar joint valgus-guided plantar inserts (Table 1).
Long-term effects of subtalar joint varus-inducing plantar inserts on subtalar joint valgus type
Although we have confirmed the immediate effect of subtalar joint varus-inducing plantar inserts on the subtalar joint valgus type of knee osteoarthritis, the long-term effects are currently unknown.
Therefore, we will confirm the long-term effectiveness of subtalar joint varus-inducing plantar inserts in one case.
Case Presentation
The case is a 70s-years-old woman who complained of pain in both knees three years ago, visited a hospital, and was diagnosed with bilateral knee OA medial type.
Her physique had a height of 156 cm, a weight of 65 kg, and a Body Mass Index (BMI) of 26.3 kg/m2. X-ray evaluation showed that the Kellgren-Lawrence (KL) grade was III on the right and III on the left, and narrowing of the joint space was observed. In addition, the femoro-tibial angle (FTA) showed marked varus deformation of 188° to the right and 187° to the left (Figure 3).
 Figure 3: X-ray image of the case.
Figure 3: X-ray image of the case.
As for the footprint, the first lateral angle was 30 degrees to the right and 26 degrees to the left, and both hallux valgus deformities were observed.
The dilatation rate was 47.9% on the right and 46.8% on the left, and both transverse arches were lowered (Figure 4).
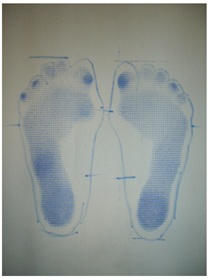 Figure 4: Footprint evaluation.
Figure 4: Footprint evaluation.
The medial longitudinal arch height rate was 11.3% on the right and 10.4% on the left, confirming low left and right arches.
The calcaneal varus/valgus evaluation was 8 degrees valgus right and 10 degrees valgus left (Figure 5). Result left and right feet was confirmed valgus flatfoot and hallux valgus.
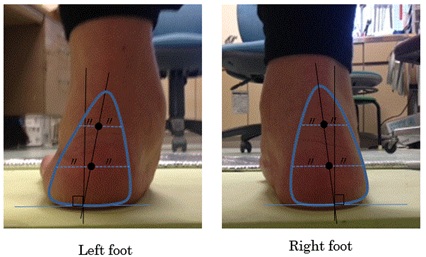 Figure 5: Right and left calcaneal valgus type case.
Figure 5: Right and left calcaneal valgus type case.
Fabrication Of Subtalar Joint Varus Guiding Plantar Insert
The sole plate was manufactured using a DSIS pad (manufactured by Sanshin Kosan Co., Ltd.) and an EMSOLD pad (manufactured by EMSOLD Co., Ltd.).
DSIS Biaxial Arch Pad®, DSIS LTW Pad®, and DSIS Heel Wedge Pad® were attached so as to cover the talus on the posterior calcaneus of the medial arch, and were manufactured to guide the subtalar joint to varus.
Using DSISLTW Pad®, DSIS Plainsheet®, and EMSOLD Metatarsal Pad®, while stacking the pads so that the calcaneus is within 2 degrees of 8 degrees of right pronation and 2 degrees of 10 degrees of left pronation. Fine adjustments were made (Figures 6 & 7).
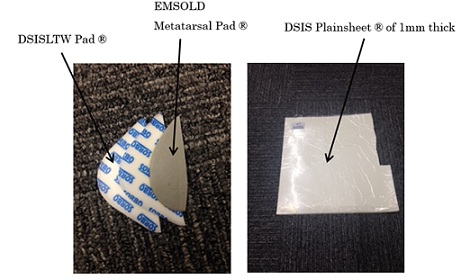 Figure 6: Calcanal varus guide adjustment pad.
Figure 6: Calcanal varus guide adjustment pad.
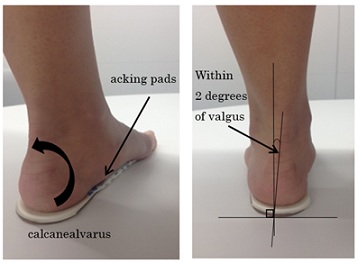 Figure 7: Setting within 2 degrees of calcaneal varus of the left foot.
Figure 7: Setting within 2 degrees of calcaneal varus of the left foot.
In addition, the counter is equipped with a soft material, EMSOLD Pad®, to hold the lateral longitudinal arch, and a DSIS forefoot wedge pad® is attached to the anterolateral side to guide kicking to the big toe (Figure 8).
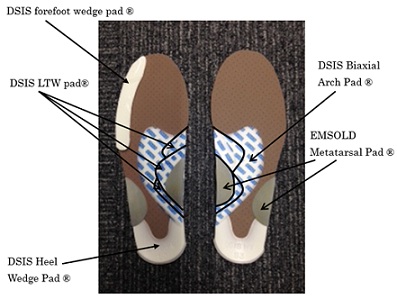 Figure 8: Subtalar joint varus-guided plantar plate for subtalar joint valgus type.
Figure 8: Subtalar joint varus-guided plantar plate for subtalar joint valgus type.
The final finish was completed by pasting No Stack Aim glue (thickness about 0.1 mm) on the surface as a finishing material made by Nintoku Trading Company.
Effect evaluation method
The insoles were evaluated by comparing the 10m maximum effort walking time and pain evaluation VAS, the total consumption and the number of steps in one week without wearing the insoles and immediately after wearing the insoles.
In order to see the long-term effect, functional evaluation was performed 3 months, 6 months, and 12 months after wearing the insoles.
Evaluation items are 10m walking time, Visual Analogue Scale (VAS) after 10m walking, hallux valgus angle (first toe side angle), number of steps with a lifestyle recorder (lifestyle recorder Lifecorder GS manufactured by Suzuken), and total consumption. Evaluation of 10m walking was performed 3 times for each measurement and compared from the average value.
The shoes used in this study had to have unworn soles and fit in size and width.
Results
The average of 3 evaluations of 10m walking was 9.9 seconds for 10m walking without plantar plate, and the VAS score was 72 points for the right knee and 70 points for the left knee.
After wearing the plantar plate the 10m walking time was 8.5 seconds, and the VAS improved to 50 points for the right knee and 40 points for the left knee.
In addition, an increase in the total amount consumed and the number of steps taken during one week of wearing the plantar plate was observed.
After 3 months, 6 months, and 12 months after wearing the plantar plate, the VAS improved to 0 points in both knees and the 10m walking time improved to 6.7 seconds.
The lateral angle of the first toe was 30 degrees to the right and 26 degrees to the left, but improved to 20 degrees to the right and 21 degrees to the left after 12 months (Table 2). The Lifecorder GS measurement results showed an average of 1954 steps and a total consumption of 1143 kcal during the first week without wearing plantar plate.
|
|
Before wearing |
3month later |
6month later |
12months later |
|
10m walking time (sec) |
9.9 |
7.7 |
7.5 |
6.7 |
|
Right VAS (points) |
72 |
10 |
10 |
0 |
|
Left VAS (points) |
70 |
0 |
0 |
0 |
|
Right 1st toe lateral angle (deg) |
30 |
29 |
26 |
20 |
|
Left 1st toe lateral angle (deg) |
26 |
24 |
23 |
21 |
|
Total monthly consumption average (kcal) |
1143 |
1646 |
1720 |
2012 |
|
Monthly average number of steps |
1954 |
2845 |
3014 |
3730 |
|
Weight (kg) |
64 |
63 |
62 |
60 |
|
BMI (kg/m2) |
26.3 |
25.9 |
25.5 |
24.7 |
|
Waist (cm) |
109.5 |
104 |
98.5 |
93 |
|
Hip (cm) |
100 |
99 |
97 |
95 |
|
body fat percentage (?) |
34.8 |
32.7 |
32 |
31.2 |
Table 2: Progress of functional evaluation by wearing plantar plate.
After 12 months of wearing plantar plate, the average number of steps was 3730 steps and the total consumption was 2012 kcal, indicating an increase in energy consumption (Table.2). Without plantar plate weight was 64 kg, BMI was 26.3 kg/m2, waist (W) was 109.5 cm, hip (H) was 100 cm, and body fat percentage was 34.8%. Twelve months after wearing the plantar plate, the weight decreased to 60 kg, BMI to 24.7 kg/m2, W to 93.0 cm, H to 95.0 cm, and body fat percentage to 31.2% (Table 2).
Consideration
Effects of subtalar joint varus-inducing plantar inserts
For subtalar joint valgus types, walking ability, balance ability, and pain were significantly improved with subtalar joint varus-guided plantar inserts than with subtalar joint valgus-guided plantar inserts.
It has also been reported that pain is less likely to change when the subtalar joint is guided from valgus to valgus [8].
It has also been stated that guiding the subtalar joint from valgus to varus induces terminal rotation of the knee and improves knee function [4,9].
Based on the above, subtalar joint varus-guided plantar inserts were considered to be more effective for the subtalar joint valgus type.
However, the subtalar joint valgus type is also said to be a physiological pain-protective response to increased FTA, and when guiding in the varus direction, care must be taken not to strengthen the guidance considering the possibility of pain [10,11].
Long-term effects of subtalar joint varus-inducing plantar inserts
The manufactured plantar plate has been suggested to be effective in the long term, and the inversion guidance of the calcaneus valgus to within 2 degrees by the plantar plate reduces pain during walking, I thought it was possible resulting in comfortable walking. For cases in which the subtalar joint is valgus, the varus guide that guides the calcaneus to within 2 degrees of valgus is used instead of the lateral wedge-type plantar plate that induces valgus of the subtalar joint1-5. The results supported the effectiveness of the varus guide plantar plate. We believe that the use of plantar plate reduced pain during walking and temporarily corrected knee movements, resulting in short-term effects. In addition, it is inferred that the longer the wearing period, the more the knee movement was improved, and the longer the effect was obtained.
Relief of pain during walking by wearing a plantar plate makes going out and walking more enjoyable, and is expected to have the effect of extending healthy life expectancy by preventing muscle weakness and obesity.
Conclusion
For the subtalar joint valgus type, subtalar joint varus-guided plantar inserts were the most effective.
When it comes to plantar inserts for knee osteoarthritis, it is important to perform individual evaluations and create plantar inserts to improve individual alignment, rather than simply prescribing a lateral wedge.
References
- Shimizu S (2008) Examination of plantar inserts therapy for hindfoot pronation and supination in knee osteoarthritis. PT Journal 42: 763-768.
- Kakihana W, Akai M, Yamasaki N, Takashima T, Nakazawa K (2004) Changes of joint moments in the gait of normal subjects wearing laterally wedged insoles. Am J Phys Med Rehabil 83: 273-278.
- Yasuda K, Sasaki T (1987) The mechanics of treatment of the osteoarthritic knee with a wedged insole. Clin Orthop Relat Res 215: 162-171.
- Uchida T (1992) Plantar inserts therapy for knee osteoarthritis -About the knee joint from the perspective of the foot-. Journal of the Tokyo Knee Joint Society 13: 168-171.
- Yan Y (1992) Lower limb alignment and subtalar joint movement. Journal of the Japanese Society of Foot Surgery 13:127-130.
- Sasaki K (1998) Plantar insert therapy for ankle joint ligament injuries. Orthopedic Plastic Surgery 41: 1225-1236.
- Ohkubo M (1995) Heel of varus and valgus and disability. Joint Surgery14: 85-93.
- Ishii S (1999) Mechanism and effects of lateral cuneiform plantar inserts on knee osteoarthritis. The Journal of Clinical Physical Therapy 2: 23-28.
- Kobayashi I (1983) Lower extremity alignment in knee osteoarthritis - pathological condition seen from gait analysis. Orthopedic Surgery Mook 29: 78-88.
- Shimizu S (2008) Relationship between pronation and supination of the hindfoot in medial type knee osteoarthritis and FTA/KL classification. Shoe Medicine 22: 11-13.
- Takeuchi R (2000) Effect of subtalar joint pronation movement on alleviating lower limb varus deformity. MB Orthop13: 1-10
Citation: Shimizu S, Hanamura H, Ida K, Katoh Y (2024) Plantar Inserts Therapy for Hind Foot Subtalar Joint Valgus Type in Medial Gonarthrosis. J Altern Complement Integr Med 10: 491.
Copyright: © 2024 Shingo Shimizu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.