Stabilization of Spontaneous Cerebral Coil Detachment with Stent during Endovascular Treatment of Direct Carotido-Cavernous Fistula: A Case Report
*Corresponding Author(s):
Reza MohammadianRadiology Department, Stradins University, Riga, Latvia
Tel:+37167000610,
Email:diako30@yahoo.com
Abstract
Carotido-cavernous fistula (CCF) is a rare vascular anomaly and endovascular treatment plays a crucial role in managing of it. However, complications can arise, including spontaneous coil detachment, which can lead to embolic or thrombotic events. In this case report, we present the case of a 56-year-old man who suffered multiple skull base and facial bone fractures, along with a traumatic subarachnoid hemorrhage, resulting from a fall. The patient was diagnosed with a right-sided traumatic carotid-cavernous fistula, and endovascular treatment with coiling was performed. During the procedure, a coil spontaneously detached, to address this complication, a stent was deployed to fix the dislodged coil to the carotid artery wall, ensuring proper occlusion and minimizing the risk of further embolic or thrombotic events. This rescue technique provides stability to the detached coil, minimizing the risk of migration or embolization, and preserves the integrity of the internal carotid artery. Spontaneous coil detachment is a challenging situation during endovascular treatment, but with proper techniques, such complications can be managed effectively, ensuring successful closure of the carotido-cavernous fistula and patient safety.
Keywords
Carotido-cavernous fistula; Coil detachment; Stent; Spontaneous
Introduction
Carotido-cavernous fistula (CCF) is a rare vascular anomaly characterized by abnormal communications between the internal carotid artery (ICA) and the venous compartments of the cavernous sinus. [1] It is commonly associated with craniofacial trauma and may present with various clinical manifestations [2,3].
Endovascular treatment plays a crucial role in the management of traumatic CCF, offering a minimally invasive approach to address this vascular abnormality. While endovascular treatment is generally considered safe and effective, several complications can arise [4].
Spontaneous coil detachment is a rare complication and can occur when the coils detach from the delivery wire or each other, potentially causing embolic or thrombotic events.
Here, we present a case of a 56-year-old man with a right-sided traumatic carotid-cavernous fistula. Endovascular treatment with coiling was performed to occlude the fistula. However, during the procedure, a coil detached spontaneously, posing a risk of thrombo-embolization. To address this complication, a stent was carefully deployed to fix the dislodged coil to the carotid artery wall, ensuring proper occlusion and minimizing the risk of further adverse events.
Case Description
The emergency department received a 56-year-old man who had suffered multiple fractures in the skull base and facial bones, as well as a traumatic subarachnoid hemorrhage, after falling from a height of around 5 meters. Further investigation, including CTA and DSA, confirmed the presence of a direct carotid-cavernous fistula on the right side. (Figure 1).
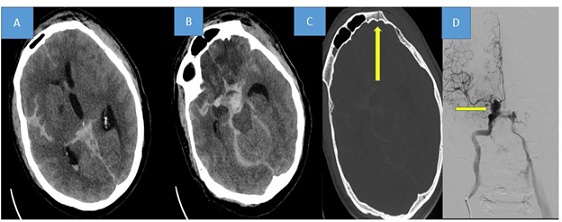 Figure 1: Brain CT scan revealing extensive subarachnoid hemorrhage (SAH) with greater prominence on the right side. (A and B). Bone view window displaying multiple bone fractures (one of them indicated by the yellow arrow) (C). Digital Subtraction Angiography (DSA) illustrating a traumatic carotid cavernous fistula on the right side (D).
Figure 1: Brain CT scan revealing extensive subarachnoid hemorrhage (SAH) with greater prominence on the right side. (A and B). Bone view window displaying multiple bone fractures (one of them indicated by the yellow arrow) (C). Digital Subtraction Angiography (DSA) illustrating a traumatic carotid cavernous fistula on the right side (D).
Considering the location of the lesion and the characteristics of the fistula, we opted for the arterial approach as the preferred method for the endovascular treatment.
To initiate endovascular embolization, the balloon assistance technique was utilized. Although the initial placement of the coils proceeded without complications, a micro-coil spontaneously disconnected while delivering a 6-10mm x 30cm coil. Retrieving the disconnected coil mechanically posed a risk of compromising the previously inserted coil cast. To prevent the occurrence of ICA thrombosis or even potential late migration, the detached portion of the coil was straightened and elongated using a thrombectomy stent measuring 6x30mm. During this process, a complete closure of the carotid-cavernous fistula was observed in the subsequent DSA. The proximal part of the elongated coil was secured using self-expandable stents measuring 7 mm x 40 mm to maintain its straightened position. A final run DSA revealed a fixed coil firmly pressed against the carotid wall by the stent, confirming the complete closure of the carotid-cavernous fistula (Figure 2).
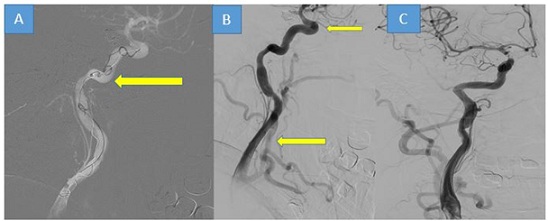 Figure 2: Image “A’’ showed the spontaneously disconnected coil in the right internal carotid artery. (Yellow arrow) The detached portion of the coil was straightened and elongated using a stent proximally and distally (yellow arrows, (B). A final run DSA revealed a fixed coil firmly pressed against the carotid wall by the stent, and complete closure of the carotid-cavernous fistula (C).
Figure 2: Image “A’’ showed the spontaneously disconnected coil in the right internal carotid artery. (Yellow arrow) The detached portion of the coil was straightened and elongated using a stent proximally and distally (yellow arrows, (B). A final run DSA revealed a fixed coil firmly pressed against the carotid wall by the stent, and complete closure of the carotid-cavernous fistula (C).
Discussion
In our presented case of post-traumatic carotido-cavernous fistula, we encountered a challenging and threatening complication: spontaneous cerebral coil detachment.
The inability to retrieve a spontaneously detached coil from the artery posed a significant obstacle, putting the patient at risk of neurological deterioration. To address this critical situation, we employed a rescue technique involving stent assistance for coil capture and fixation at the vessel wall.
Through our technique, we successfully stabilized the detached coil by straightening and elongating it using a thrombectomy stent. The proximal part of the stretched coil was fixed against the vessel wall with self-expandable stents, ensuring proper coil apposition and closure of the carotido-cavernous fistula. By straightening and elongating, we achieved stabilization of the detached coil and preservation of the internal carotid artery.
Spontaneous cerebral coil detachment poses a significant challenge during the endovascular treatment of complex lesions, such as arterio-venous fistulas. The most concerning consequence is the migration of the detached coil to a distal artery. Coil migration during the treatment of complex cerebral vascular lesions has been reported and can give rise to various complications. These complications may include stroke, recurrence of the lesion, or the occurrence of local mass effect [5-9].
One of the key difficulties in managing a spontaneously detached coil is the inability to retrieve it from the artery. Mechanical evacuation techniques were deemed impractical such as our case, due to the risk of compromising the previously inserted coil cast.
To address this situation, we employed a rescue technique utilizing stent assistance. This approach proved to be effective in preventing the risk of internal carotid artery (ICA) thrombosis and allowed for the preservation of ICA integrity even in urgent cases [10].
The use of stent assistance for coil capture and fixation at the vessel wall has demonstrated its value in avoiding threatening complications and achieving higher success rates in similar cases [11,12].
This approach provides stability to the detached coil, minimizing the risk of migration and embolization.
Conclusion
Spontaneous cerebral coil detachment during the endovascular treatment of complex lesions, such as post-traumatic carotido-cavernous fistula, presents a challenging and potentially dangerous complication. Retrieving the detached coil from the artery is not always feasible, emphasizing the need for effective rescue techniques.
The use of stent assistance in such cases has shown promising results, providing a valuable tool to prevent threatening complications and improve treatment outcomes. Tailoring the endovascular approach to individual cases based on the specific characteristics of the detached coil, pathology type, and anatomy is crucial for successful management.
Acknowledgments
None.
Ethics Statement
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Fund
None.
Author Contributions
R.M, I.K and S.P contributed to the conception and design of the study. S, P performed the endovascular procedure. A.K, S.P and I.K analyzed and interpreted the patient data. R.M drafted the manuscript. All authors critically reviewed and approved the final version of the article.
References
- Henderson AD, Miller NR (2018) Carotid-cavernous fistula: current concepts in aetiology, investigation, and management. Eye (Lond). 32: 164-172.
- Schütz P, Bosnjakovic P, Abulhasan YB, Al-Sheikh T (2014) Traumatic carotid-cavernous fistula in a multiple facial fractures patient: case report and literature review. Dent Traumatol. 30: 488-492.
- Jimenez DF, Gibbs SR (1995) Carotid-cavernous sinus fistulae in craniofacial trauma: classification and treatment. J Craniomaxillofac Trauma. 1: 7-15.
- Alatzides GL, Opitz M, Li Y, Goericke S, Oppong MD, et al. (2023) Management of carotid cavernous fistulas: A single center experience. Front Neurol. 14: 1123139.
- Aoun SG, Rahme RJ, El Ahmadieh TY, Bendok BeR, Hunt BH (2013) Incorporation of extruded coils into the third nerve in association with third nerve palsy. Journal of Clinical Neuroscience. 20: 1299-1302.
- Cherian M, Mehta P, Hedgire S, Kalyanpur T (2010) An unusual case of coil migration. A case report. Neuroradiol J. 23: 363-367.
- Rebchuk AD, Gooderham PA, Okhovat S, Janjua AS, Heran MKS (2022) Delayed coil migration into oropharynx following endovascular coiling of a traumatic carotid cavernous fistula: management considerations. Acta Neurochir (Wien). 164: 1287-1292.
- Haley M, Kumaria A, Lenthall R, McConachie N, Smith S, et al. (2020) Coughing on the coil; a case report and literature review of eight cases of endovascularly treated ICA pseudoaneurysms with coil migration into the oropharnyx. British Journal of Neurosurgery. 1-3.
- Zhuang Q, Buckman CR, Harrigan MR (2007) Coil extrusion after endovascular treatment. Case illustration. J Neurosurg. 106: 512.
- Dedmon M, Meier J, Chambers K, Remenschneider A, Mehta B, et al. (2014) Delayed Endovascular Coil Extrusion following Internal Carotid Artery Embolization. J Neurol Surg Rep. 75: 255-258.
- Schütz A, Solymosi L, Vince GH, Bendszus M (2005) Proximal stent fixation of fractured coils: technical note. Neuroradiology. 47: 874-878.
- Abdelrady MM, Ognard J, Abdelsamad AM, Mahmoud M (2022) Parent artery stenting as a rescue management for stretched coils during cerebral aneurysms embolization: Report of three cases and review of literature. Interv Neuroradiol. 28: 613-622.
Citation: Ponomarjova S, Karimova I, Kratovska A, Mohammadian R (2024) Stabilization of Spontaneous Cerebral Coil Detachment with Stent during Endovascular Treatment of Direct Carotido-Cavernous Fistula: A Case Report. J Clin Stud Med Case Rep 11:215
Copyright: © 2024 Sanita Ponomarjova, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.