Subcutaneous Emphysema and Pneumomediastinum - Investigating Chest Pain
*Corresponding Author(s):
Gabriela ReisDepartment Of Pediatrics, Hospital José Joaquim Fernandes, Unidade Local De Saúde Do Baixo Alentejo, Beja, Portugal
Abstract
Chest pain is a common cause of observation of children and adolescents in emergency departments; however, it is important por clinicians to accurately diagnose and promptly treat serious conditions.
The authors present a rare case of 14-year-old teenager with a history of chest pain and subcutaneous emphysema, to raise awareness for potentially life-threatening causes of thoracic pain
Keywords
Chest pain; Emphysema; Pneumomediastinum; Pneumothorax
Case Presentation
Previously healthy, non-smoker, 14-year-old girl, presented to the emergency department with sudden onset of pain on the left side of the neck and upper thorax. She had no personal history of respiratory disease and was not on any regular medication. Although the patient denied any trauma, she recalled an episode of lifting a heavy mattress two days earlier.
Initial observation showed she was a febrile, hemodinamically stable and had oxygen saturation levels of 98% on air.
On examination, heart and pulmonary sounds were normal. She had slight cervical subcutaneous emphysema with crepitus on palpation.
From the additional study, blood tests had no elevation of inflammatory parameters. Chest radiography showed cervical subcutaneous emphysema, suggesting the possibility of Pneumomediastinum (Figure 1).
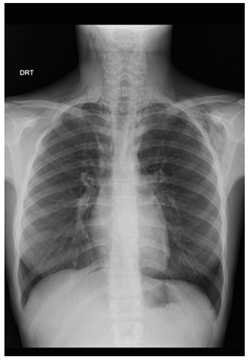 Figure 1: Chest radiography revealing cervical subcutaneous emphysema. Pneumomediastinum may be seen, extending into the neck and outlining the pericardium.
Figure 1: Chest radiography revealing cervical subcutaneous emphysema. Pneumomediastinum may be seen, extending into the neck and outlining the pericardium.
She underwent CT-Scan, which revealed widespread emphysema, that dissected the laterocervical mucle-aponeurosis plans from the skull base to the supraclavicular fossa, on the right, and the shoulders, on the left (Figure 2). The exam showed the presence of pneumomediastinum and bilateral pneumothorax (Figure 3).
 Figure 2: Cervical and thoracic CT-Scan (coronal, non-contrast) demonstrating extensive emphysema extending through the neck, from the cranial base to the supraclavicular fossa, on the right and the shoulders, on the left.
Figure 2: Cervical and thoracic CT-Scan (coronal, non-contrast) demonstrating extensive emphysema extending through the neck, from the cranial base to the supraclavicular fossa, on the right and the shoulders, on the left.
 Figure 3: Chest CT-Scan (axial, non-contrast) showing extensive pneumomediastinum and bilateral small blades of pneumothorax. No tracheal perforation. Heart and aorta within normal limits.
Figure 3: Chest CT-Scan (axial, non-contrast) showing extensive pneumomediastinum and bilateral small blades of pneumothorax. No tracheal perforation. Heart and aorta within normal limits.
She was admitted as inpatient under oxygen therapy, for clinical and radiological monitoring. The patient was discharged after five days, asymptomatic. She has been regularly reviewed as an outpatient, and after six months, she’s had no further symptoms. No specific cause has been identified [1].
Discussion/ Conclusion
Spontaneous pneumomediastinum, a rare condition in pediatrics, is defined by the presence of free air within the mediastinum, as the result of a sudden increase in intraalveolar pressure. This leads to rupture and leak of air, which reaches the hilum and spreads into subcutaneous tissues, causing subcutaneous emphysema [2-3].
This condition usually occurs in healthy patients; following Valsalva’s maneuver [3], and is not associated with trauma. Although chest pain is a common cause of observation in the emergency room, clinicians should always keep a high level of suspicion for severe conditions.
References
- Jindal A, Singhi S (2011) Acute chest pain. Indian J Pediatr 78: 1262-1267.
- Tortajada-Girbés M, Moreno-Prat M, Ainsa-Laguna D, Mas S (2016) Spontaneous pneumomediastinum and subcutaneous emphysema as a complication of asthma in children: case report and literature review. Ther Adv Respir Dis 10: 402-409.
- Chalumeau M, Le Clainche L, Sayeg N, Sannier N, Michel JL, et al. (2001) Spontaneous pneumomediastinum in children. Pediatr Pulmonol 31: 67-75.
Citation: Reis G, Mendo T, Rocha FN, Seves MG (2022) Subcutaneous Emphysema and Pneumomediastinum - Investigating Chest Pain. J Clin Stud Med Case Rep 9: 0131.
Copyright: © 2022 Gabriela Reis, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.