The Peaks and Troughs of Vancomycin Compliance
*Corresponding Author(s):
Tracy O'BrienFaculty - Assistant Professor Of Nursing , University Of Pittsburgh, Pennsylvania, United States
Email:TAO67@pitt.edu
Abstract
Background
Vancomycin is a powerful antibiotic that is used to treat many infections. The monitoring of this medication (peak and trough) is extremely critical to its effectiveness. Vancomycin discrepancies have increased by 17.4% over 15-months.
Aim
The aim is to decrease Vancomycin protocol discrepancies through education and surveillance on two nursing units.
Methods
Study design is a two-phase, pre/post intervention chart review of patients ordered Vancomycin and education of nursing staff. Data was collected from all full-time, part time, and casually employed registered nurses on a Medical/Surgical Unit and a Progressive Care Unit during a pre-quiz was given prior to education session and followed by a post quiz. Another post three-month quiz was administered to the same staff. Vancomycin discrepancies were monitored for three months preceding education and three months post education to monitor the discrepancies compared to the patients that were ordered Vancomycin.
Results
There was a statistically significant difference between pre-quiz / post quiz scores (p<0.0001). There was a statistically significant difference between post- and 3-month errors (p= 0.002).
Regarding Vancomycin Protocol Discrepancies, there was no statistically significant association (p-value = 0.84) on the Medical/Surgical Unit but there was a significant statistically association Χ2 = 4.89 (p-value = 0.03) on the Progressive Care Unit.
Conclusion
The discrepancy rate for Vancomycin decreased after the education in-service for nurses. Therefore, ongoing education is needed for nurses to recognize the importance of Vancomycin compliance. It is vital that physicians and pharmacists are included in future educational endeavors.
Introduction
Vancomycin is a powerful antibiotic that is used to treat many infections. The monitoring of this medication is extremely critical to its effectiveness. The complexity of dosing of this drug is based on weight initially. The exact dosage adjustments are continued according to trough levels in the blood. This is where the lowest level of the drug is present. This is obtained 30 minutes prior to the next scheduled timed dose. The problem continues to affect therapeutic drug monitoring in serum concentrations of the drug [1]. Vancomycin is used in lieu of penicillin in some cases to treat and prevent various bacterial infections caused by gram- positive bacteria, including Methicillin-Resistant Staphylococcus Aureus (MRSA) as well as effective treatment for streptococci, enterococci, pneumonia, sepsis, and cellulitis infections [2]. This has been identified as a quality and safety opportunity and reviewed with pharmacy consisting of missed laboratory tests and retimed medications outside of the safe administration window.
Problem Description and Significance
At a tertiary hospital shown in Pittsburgh, Pennsylvania, the discrepancy rate from July 2022-September 2023 showed on two patient care units (Medical/Surgical and Progressive Care), 138 medication orders for Vancomycin were completed. Out of those 138, the medication discrepancy reports voluntarily filed total 24. Thus, 17.4% of discrepancies related to Vancomycin discrepancies were due to retiming of dose, an expired drug, and missed window for obtaining accurate peak and trough levels. This causes a misrepresentation of the trough concentration if the drug is not administered at the proper time and/or the level is not drawn at the correct time. There are no benchmarks found nationally or in-house for Vancomycin. A 2018 study revealed that less than 25% of trough levels were drawn within true trough times [3]. Once the trough level was added to medication administration record, the outcomes were evaluated before (retrospective group) and after (prospective group) implementation of this initiative [3]. The study reveals patients for whom a Vancomycin level was drawn, 24.0% of patients in the retrospective group had their first Vancomycin level drawn within 2 hours of true trough, compared with 87.2% of patients in the prospective group (p < 0.0001) [3]. With a delay or untimely delivery of Vancomycin, this will add additional expenses such as laboratory tests and medication. Furthermore, levels that are too high can lead to renal toxicity and even progress to renal failure or a need for dialysis. Levels that are too low can lead to subtherapeutic treatment, worsening infection. Also, the impact of mistimed trough levels can lead to improper dosing and extended length of stay [4]. Hospital daily costs vary per state.
According to Davis [5], The average hospital stay is 4.6 days. At an average cost of $2,873 a day, Americans need to work many hours to cover these expenses. The duration of therapy for treatment of Methicillin-Resistant Staphylococcus Aureus (MRSA). Skin Infections, such as cellulitis, may range from 5 to 14 days depending on the extent of infection and response to current anti-infective therapy [6]. Therefore, it is imperative that Vancomycin be given in a prompt fashion with accurate peak and trough levels.
Vancomycin administration discrepancies may lead to an extended hospital stay for patients. Hospital daily costs vary per state. According to Davis [5], The average hospital stay is 4.6 days. At an average cost of $2,873 a day, Americans need to work many hours to cover these out-of-pocket, added expenses of additional days in the hospital. The duration of therapy for treatment of Methicillin-resistant Staphylococcus aureus and skin infections, such as cellulitis, may range from 5 to 14 days depending on the extent of infection and response to current anti-infective therapy [6]. A study cited in VanDort et.al. [7] indicated that education in hospitals is done generally on antimicrobials but not specifically on the importance of Vancomycin, which could improve therapeutic monitoring of the drug with healthcare professionals. The goal of this Evidence-Based Quality Improvement (EBQI) project is to find a successful way to safely improve monitoring and dosing of Vancomycin.
Available Knowledge
One study by Peyko and Friedman-Jakubovics [3], shows two groups being evaluated for Vancomycin trough compliance. The retrospective group held all patients who received Vancomycin between January 27th through April 26th of 2015 and the perspective group were prescribed from March 14th through June 14th of 2016 [3]. Out of the 228 patients, 24% of patients in the retrospective group had a true trough level drawn Peyko and Friedman-Jakubovics [3]. This brings to light, based on this study and others, that poor compliance is in effect at many facilities. The goal of this project is to find a successful way to safely improve monitoring and dosing of Vancomycin.
This study was a comparison of two groups that showed a multidisciplinary approach to Vancomycin trough monitoring involving automatic generation of trough orders, pharmacist. validation of trough orders, and inclusion of trough orders in the nursing medication administration record was successful in significantly improving timing of Vancomycin trough levels [3]. It reflected a retrospective group (n = 228) prospective group (n = 199). It was conducted at an 864-bed teaching hospital at Kingsbrook Jewish Medical Center in Brooklyn, NY, forming 326-acute care beds and 538 long-term care beds. [3]. This was a larger facility compared to the community hospital this writer is evaluating. According to Peyko and Friedman-Jakubovics [3], all patients for whom a Vancomycin level was drawn, 24% of patients in the retrospective group had their first Vancomycin level drawn within 2 hours of true trough, compared with 87.2% of patients in the prospective group (p < 0.0001).
In addition to the earlier research, this exploration was also at a larger hospital and the intervention stayed the same. The trough level was placed on the medication administration record. Although there is conflicting data regarding the clinical benefit of an EMR, one chronicle has found the EMR improves patient care by decreasing length of stay and mortality [4]. Variables remain consistent throughout all studies regarding timing of levels, which 2597 Vancomycin levels were assessed. In this study, 41.3 % of the specimens were drawn too early. Of the levels eligible for inclusion, 331 were in the pre-intervention period and 297 were in the post-intervention period. Levels in the post-intervention group using the Vancomycin MAR level order were less likely to be missed or drawn at an incorrect time (11.1 % vs 36 %, p < 0.01) and were less likely to require rescheduling (3.4 % vs 8.5%, p < 0.01) [4]. These samples yielded significantly higher mean Vancomycin levels than correctly timed samples [4]. Based on all reviews, Shah et al. [4] concluded that utilization of a Vancomycin MAR level order was associated with a significant decrease in incorrectly drawn Vancomycin levels.
Subsequently, Mishra et al. [8] had a similar study with automating Vancomycin orders for better monitoring. Mishra et al. [8] showed the frequency of trough levels drawn between the third and fourth dose increased from 58.6% to 75.8% (p <0.01). However, the percentage of trough levels drawn within one hour of the fourth dose remained unchanged, possibly because nursing staff waited for the result of the level prior to administering the next dose of Vancomycin (Mishra et al., 2019).
In a study conducted by Tung [9] focused more on the timing of the medication and the difference with therapeutic monitoring. Time discrepancies in administration and monitoring were documented that patient harm may be possible. Fortunately, there was no documented harm monitored in the study. Analysis revealed a start time discrepancy ranging from 124 to 194 minutes. Tung et al. [9] study showed 19.1% had infusion start time discrepancy more than 10 minutes. Of the 487 infusion interruptions, 2.5% lasted for more than 20 minutes before the infusion resumed, 24.2% (312 of 1,287) of 1-hour infusions and 32% (114 of 359) of 2-hour infusions had over 10-minute completion time discrepancy. A total of 487 infusion interruptions were identified [9]. The education that this Researcher hopes to achieve with education and policy awareness can aid with discrepancies in administration and monitoring. Per Tung et al. [9], Clinical Decision Support (CDS) tools for Vancomycin Therapeutic Drug Monitoring (TDM) have been increasingly recommended to enable individualized precision dosing, and they are most likely to utilize data entered in the EHR to inform dosing decisions.
In a study conducted by Abdel Jalil et.al [10] at Jordan University Hospital (JUH), Vancomycin discrepancies were identified between the recorded and actual times of dose administration were noted in 83.9% of audited occasions. In comparison, such discrepancies were noted in 82.7% of audited times of sample collection. In the present study, the nurses were aware that recorded times were inaccurate. The nurses stated they were aware of the incorrect times but needed to accomplish their tasks due to work pressure.
VanDort et al. [7] focused on the education of Vancomycin monitoring. It was realized that the education needed to be specifically dedicated to this drug. This study was dedicated to physicians and nurses to identify what methods were warranted as teaching methods. Many surveyed staff preferred a multimodal approach which included interactive modules, educational meetings, handouts, frequent reminders, and in-services. Although large presentations were also reported as effective, there was not anything specific on Vancomycin noted, only antimicrobials.
In summary, the previous studies regarding Vancomycin administration reveal that by adding the laboratory monitoring levels to the medication administration records can promote compliance with therapeutic monitoring of the medication. This is a shared goal with this researcher. Currently, the facility is utilizing a “sidebar” feature in the electronic medical record to alert the nurse of any laboratory monitoring that is needed for administration. Education specifically for Vancomycin is needed upon orientation and ongoing to maintain competency and knowledge on therapeutic drug monitoring.
Evidence-Based Model
The Iowa Model was the foundation for my education. It utilized the steps in planning that were needed to provide the frontline staff learning. The Iowa Model as listed in Melnyk & Fineout-Overholt [11] consisted of distinct levels that compared to my clinical concern. The problem that has been identified was an increased number of Vancomycin medication discrepancies. This was identified through nursing huddles on the patient units and through medication safety committee reporting. It caused alarms for the pharmacy department which in turn alerted nursing via the safety committee. The following step consisted of whether these discrepancies were a priority of the organization. This concern has been forthcoming for some time with the ability to cause significant patient harm. The drug is examined very closely with pharmacokinetic monitoring through lab work. This drug is classified as a vesicant and is most effective in a narrow therapeutic window [12]. Discrepancies in administration and monitoring of this medication has led to increased length of stay for the patient. A study by Sault et.al., [13] showed that 77% of medical centers were still using trough-based monitoring and that the main barrier to the implementation of AUC monitoring was a lack of knowledge as well as lack of time and frequent errors of timing of samples. As a result of these inconsistencies, Zonozi et al. [14] show patients with an elevated trough level yielded longer average duration of Vancomycin therapy (6.0 days vs. 3.4 days vs. <1 days, p<.001) increasing risk for acute kidney injury and longer length of stay.
Form a Team
Shortly after the problem had been determined as a priority, a responsible party had to formulate a leadership team to educate the nursing staff and determine any policy and procedure discrepancies that are occurring. As a doctoral student, the medication safety committee appointed me as the Researcher for finding the discrepancies related to nursing administration and therapeutic monitoring of Vancomycin. The team consisted of the Director of Nursing, a Lead Pharmacist, Patient Safety, and the Quality Manager, as well as the management team on the designated units. The external and internal evidence continued to be reviewed and assessed regarding Vancomycin monitoring through the voluntary discrepancy reporting system.
Subsequently, leading to the need for re-education on the policy.
Design and Pilot the Education
The Vancomycin policy is in place in the network electronic policy manual. However, the hospital is experiencing generalized discrepancies with Vancomycin on all units. The discrepancy rate from July 2022-September 2023 showed on two patient care units (Medical/Surgical and Progressive Care), 138 medication orders for Vancomycin were completed. Out of those 138, the medication discrepancy reports voluntarily filed total 24. Thus, 17.4% of discrepancies related to Vancomycin discrepancies were due to retiming of dose, an expired drug, and missed window for obtaining accurate peak and trough levels. The Researcher chose two units randomly-the medical/surgical unit and the progressive care unit (with pharmacy approval) and provided in-depth education regarding the policy and procedure pertaining to Vancomycin administration and monitoring. The Researcher created a ten-question multiple choice quiz produced from the policy and procedure guidelines. This quiz was validated and edited by two licensed pharmacists in the organization. Vancomycin discrepancies were monitored on these two units for three months prior to education. The Researcher administered a pre-session quiz to test knowledge prior to education. A post-session quiz was administered after the education as well. Monitoring continued for the Vancomycin inconsistencies with policy and procedure management for three months following the last education session.
Specific Aims
The purpose of this project is to find a solution for a therapeutic drug monitoring process for Vancomycin. The current policy of peak and trough levels on the work list in the electronic medical record are missed and/or retimed by nursing. One solution proposed in the literature is that the peak and trough level for Vancomycin should be added to the MAR for better visibility for the nurses. In a previous study by Peyko and Friedman-Jakubovics [3], the same intervention at a large teaching hospital was performed. In that study, the Information Technology (IT) Department added a “dummy order” for the necessary timed-labs to the medication record with the Vancomycin [3]. Based on this 2108 study, the monitoring for Vancomycin was split between two groups: In the pre- intervention group 184.9 ± 84.8 minutes versus 58.3 ± 60.7 minutes in the post-intervention group. This would become visible for the nurses to obtain prior to administration. The goal is to increase compliance with therapeutic drug monitoring levels. If implementation of this intervention can occur, Vancomycin trough monitoring involving automatic generation of trough orders, pharmacist validation of trough orders, and inclusion of trough orders in the nursing medication administration record may be successful in significantly improving timing of Vancomycin trough levels [3].
As part of the EBQI project, this process has been requested via a Criticality Report to the Informatics Committee at the Community Hospital. The literature was submitted with the report for review. The Researcher proposed the electronic Medication Administration Record (MAR) change to include the peak and trough levels on the MAR to the leadership and Informatics Council at this Community Hospital. This concept was well received, especially by the Director of Pharmacy. He confirmed that this process had been successful at another facility prior to employment at this hospital. They also utilized the same eMAR system. At the request of the directors, this Researcher has been requested to present this innovation to the Hospital Network Leadership Teams to impose a network change throughout all their working eMAR systems. While this network change is under review, an education process was developed by the Lead Pharmacist and this Researcher developed to reiterate the importance of the Vancomycin administration and monitoring process. The facility and the EPIC electronic medical record system utilized the “sidebar” feature that does alert the nurse when the monitoring level is due.
This is an improvement to the earlier monitoring in this system where there was an independent “work list.” The prospective intervention by the Researcher was to include the peak and/or trough levels on the medication administration record as an order for the nurses to view. The addition of the “sidebar” has satisfied the need currently. Currently, the classification ‘medication discrepancies’ from July 1, 2022- February 28, 2023, consisted of 138 Vancomycin prescribed orders on studied units with Vancomycin discrepancies totaling 24. That percentage equals 17.4%. This researcher believes that implementation of this intervention at this community hospital may benefit from an increase in therapeutic drug monitoring of Vancomycin by decreasing the discrepancies hospital wide.
Rationale
The common pattern that exists in all the present studies lists medication errors based on improper management of monitoring. Nurses are not permitted to alter the administration times of the Vancomycin. Krukas et al. [15] confirmed that difficulties were noted when doses and/or timing needed to be adjusted, including starting, restarting, and stopping IV Vancomycin. Of the 39 events occurring during the monitoring medication-use process stage related to Appropriate Therapy Management, two-thirds (n=25 of 39, 64.1%) resulted in monitoring medication errors [15]. Another flaw in the monitoring system is the timed- trough levels. The levels are shown only on a work list. By adding the levels that are due to the frequently viewed Medication Administration Record (MAR), this has been shown to increase compliance. Shah et al. [4] concurred that use of a Vancomycin MAR level order was associated with a significant decrease on incorrectly drawn or missed Vancomycin levels.
Context
Setting
This EBQI project will take place in a community hospital located in Pittsburgh, Pennsylvania. This 356-bed hospital admits many specialties ranging from Cancer, Cardiovascular, Women’s’ Health, Medicine, Orthopedics and Wound Care. The current facility policy for Vancomycin practice is as follows:
- MD enters order for Pharmacy to dose Vancomycin
- Nursing should have an admission weight (actual) charted in EPIC (electronic medical record).
- Pharmacy retrieves the admission weight, places order for the loading dose, maintenance doses, Vancomycin peak and trough levels, monitors lab results, and adjusts maintenance doses based upon results.
- Nursing is to follow orders for Vancomycin peak and trough via the worklist in EPIC, administer the medication as ordered and as scheduled. Document accurately. If there is any change needed to the schedule of the medication or the Vancomycin peak and trough, the registered nurse is to notify pharmacy so the orders can be adjusted.
The initial team that will be pioneering this effort will consist of pharmacists, quality improvement, patient safety, physicians, registered nurses, and educators.
The prospective intervention would be to include the peak and/or trough levels on the medication administration record as an order for the nurses to view. This order will be populated by the pharmacy department upon receipt of the new order by physicians. Prior to the intervention being implemented, nursing will be supplied education by the Researcher. Ongoing education will be reinforced by the nurse educators, assistant, and general managers on their perspective units. The goal is to increase compliance with therapeutic drug monitoring levels. This will be measured by a decrease in the voluntary electronic discrepancy reports for the Vancomycin administration and monitoring.
Participants
Education will be provided by the Researcher to all regularly employed registered nurses on two patient units. The total number of nurses will be 28. The pharmacy department determined that the discrepancies were throughout the hospital. The units chosen to begin the education process were not the lowest or the highest number of incidents. This was the starting point only.
IRB Review Process
The study was not considered eligible for IRB approval at the Community Hospital. The only approval needed was a signed letter of intent from the New Knowledge and Innovations Council for authorization of the quality improvement project by the facility directors. An IRB proposal was presented and approved by the IRB Review Board at Carlow University.
Methods
The Vancomycin policy was in place. The hospital was experiencing generalized discrepancies with Vancomycin. The Researcher chose two nursing units randomly to supply in- depth education regarding the policy and procedure pertaining to Vancomycin administration and monitoring. The literature did not yield a reliable and validated tool. The Researcher created a ten-question multiple choice quiz produced from the policy and procedure guidelines. This quiz was validated and edited by two licensed pharmacists in the organization. Vancomycin discrepancies were monitored on these two units for three months prior to education. The Researcher administered a pre-session quiz to test knowledge prior to education. A post-session quiz was administered after the education session also. Monitoring continued for the Vancomycin inconsistencies with policy and procedure management for three months following the last education session.
The training sessions for all registered nurses will include the following list.
- The purpose of this education is due to a lack of adherence to Vancomycin administration policy and therapeutic monitoring identified by patient safety and
- A pre-test containing ten questions will be administered with a unique identifier prior to the start of the First letter of father’s first name (A–Z), First letter of mother’s first name (A–Z), Birthday – “01–31”, and Birth month – “01–12”.
- The training sessions are mandatory and will begin June 15, 2023-June 30, Sessions will be scheduled according to work schedule posting on unit.
- The number of registered nurses varied during sessions depending on time of day and activity on the unit. Average 3-4 RNs per session until all twenty-eight have been educated.
Included in the sessions:
- At the beginning of the shift, verify patient orders and who is on
- Confirm that the actual height and weight are documented, and a serum creatinine was obtained. These are absolute requirements and must be documented for Vancomycin dosing to occur.
- Check orders each shift for laboratory orders related to Vancomycin – peak, trough, or random.
- Review daily monitoring note(s) from pharmacy which are available in the progress notes in electronic medical record for updates.
- Read any associated administration instructions that may be on the actual Vancomycin order itself.
- Explain the narrow therapeutic window for effectiveness of this drug and why timing is crucial.
- Hemodialysis patients: Vancomycin should always be administered after dialysis is completed.
- Trough levels are drawn 30 minutes before administration of Peak levels are drawn 60 minutes after completion. Do not hold doses waiting for results.
- Pharmacy should be notified immediately with:
- Any deviation or change from established Vancomycin administration times must be communicated to pharmacy
- Doses must be administered within 60 minutes for
- Initial dose or loading dose of Vancomycin is ordered to be given STAT and should be administered promptly, approximately 30 min after order placement and/or drug received on the unit.
- Any loss of IV access or any reason that may cause delays in administration should be communicated as soon as possible to the
- Any missed lab draw should be communicated as soon as possible to pharmacy.
- Compliance of Therapeutic Vancomycin Monitoring will occur following the completion of educational sessions beginning July 1, 2023- September 30, This will continue with the monitoring of discrepancy reports.
- A post-test after three months following the education session will be administered to the same participants with the same unique identifiers in the first two weeks of October 2023 to solidify obedience with the policy and procedures surrounding Vancomycin. If post-test is less than 100%, re-education on the policy will occur at that time.
Interventions
The intervention based upon earlier research to improve the outcome of missed peak and/or trough levels, or retimed doses during Vancomycin treatment is to add reminders for lab draws on to the medication records. Meetings occurred between the Researcher and Information Technology Team and Pharmacy Directors with proposals. Currently, the lab work reminders show on a separate work list. There was hesitancy from the network team to agree to the MAR addition. As a result, there was a middle ground started in EPIC called the Sidebar. It shows the work list simultaneously with the MAR. This does make it easier and more convenient to know when peak and trough levels are due. This has been in effect during the three-month post- monitoring of discrepancies. All stages of the project are the responsibility of the Researcher.
The first stage is initiating the evidenced-based quality improvement project. This was started by identifying the lapse in education regarding the Vancomycin policy.
The planning of the project was discussed in detail with scheduled meetings with the Director of Nursing, Manager of Nursing Quality, and Lead Pharmacist working closely with the Vancomycin Task Force for error reduction. Planning was also discussed with the Course Faculty Advisor at Carlow University for approval. The EBQI project proposal was approved by the Internal Institutional Review Board (IRB) at Carlow University. The Community Hospital did not require internal approval as it was a Quality Improvement Project. This plan consisted of formal education of 30 minutes with 3-6 nurses with review of policy, pharmacokinetic procedure for Vancomycin, a question-and-answer session and pre and post quiz.
Education began June 15, 2023-June 30, 2023, and continued until all nurses had been educated on the two pre-selected units. The results of the Vancomycin discrepancies will be reviewed by the voluntary error reporting system. A lower percentage rate is anticipated after education. Ongoing education will be performed by the unit manager, educators, and annual education.
Education for the nurses regarding Vancomycin compliance and monitoring focused on the need for strict timing for laboratory monitoring. The window for accuracy is very small. The risk of nephrotoxicity is a possibility with improper monitoring and abnormal laboratory levels. The need to provide additional support is warranted.
The consensus of the referenced literature continues to support this intervention for increased acceptance of the newly acquired addition to the process. By adding the laboratory levels to the medication administration records has shown improvement in previous studies. According to Peyko and Friedman-Jakubovics [3], the assigned groups in the study showed a significant increase in compliance with trough levels with automated orders being placed on the medication administration records.
As noted by Shah et al. [4], A total of 1353 Vancomycin levels were assessed, and 628 levels met inclusion criteria. The utilization of Vancomycin MAR level order was associated with a significant decrease in incorrectly drawn Vancomycin levels.
Lastly, Mishra et al. [8] studied that automating monitoring orders with medication orders decreased missed levels. The trough was automatically entered onto the medication administration record prior to the fourth dose of Vancomycin [8]. It was confirmed that a decrease in missed levels with MAR inclusion. The work was deemed successful in the medical center.
Therefore, previous studies have shown success with automation monitoring orders to the MAR. This current proposal would begin with the physician order for the medication. Nursing will ensure that a current actual weight is obtained and entered in the record. Pharmacy will then begin the pharmacokinetic procedure for dosing and assigning orders and levels to the medication administration record. Currently the MAR contains bold reminders to verify levels. However, by adding a peak and/or trough order to the actual MAR to sign-off, it is less likely to be omitted as more nurses visualize the medication record more frequently than the work list. The Information Technology Department has begun utilizing a “sidebar” feature that shows that worklist parallel to the MAR for easier access.
Education
Baseline measurements for discrepancies were obtained through the online electronic reporting system. The discrepancies were tabulated and evaluated to form an educational platform for nursing to facilitate understanding of the processes regarding the importance of the Vancomycin procedure.
The education was created with the Researcher and Lead Pharmacist to develop the education based on key features that have been reported as ongoing discrepancies. The education was provided to two separate nursing unit staff based on the frequency of discrepancies from reporting and pharmacy discretion. The sessions were approximately 30 minutes in length.
Training sessions will begin June 15, 2023-June 30, 2023. There will be a pre- and post- quiz. An incorrect score will be remediated for accuracy. The number of registered nurses varied during sessions depending on time of day and activity on the unit. Information was presented that included:
- At the beginning of the shift, verify patient orders and who is on
- Confirm the actual height and weight are This is an absolute requirement and must be documented for Vancomycin dosing to occur.
- Check orders each shift for laboratory orders related to Vancomycin – peak, trough, or random.
- Review daily monitoring note(s) from pharmacy which are available in the progress notes for updates.
- Read any associated administration instructions that may be on the actual Vancomycin order itself.
- Hemodialysis patients: Vancomycin should always be administered after dialysis is
When to notify Pharmacy immediately:
- Any deviation or change from established Vancomycin administration times must be communicated to pharmacy staff. Doses must be administered within 60 minutes for accuracy.
- Initial dose or loading dose of Vancomycin is ordered to be given STAT and should be administered promptly, approximately 30 min after order placement and/or drug received on the unit.
- Any loss of IV access or any reason that may cause delays in administration should be communicated as soon as possible to the pharmacy.
- Any missed lab draw should be communicated as soon as possible to Pharmacy.
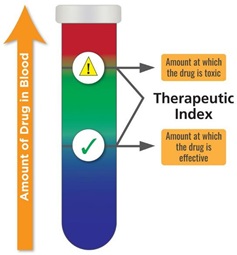
Education will explain why this process is so important and does not allow for great deviation. To oversimplify it is because of the narrow therapeutic index of Vancomycin and what could go wrong if levels are too high (or too low) [16].
Now that all the education is completed, monitoring of the electronic reporting system will continue. Problems that arose were scheduling conflicts such as vacations, scheduled off days, leaves of absences, separation of employment, and call-offs. Patient acuity and staffing needs also dictated scheduling opportunities. The Researcher made every attempt on every shift to accommodate schedules for all registered nurses. Education sessions were completed in 2.5 weeks [17].
Analysis
Data was obtained by pre, post, and post three-month quiz scores. All scores (n=28) were added to an Excel Spreadsheet for analysis. All separate quiz values were used [18]. A Wilcoxon Signed Rank Test (non-parametric version of paired t-test) was performed to test if there was a difference between the number of incorrect quiz answers [19]. There was a statistically significant difference between pre and post quiz answers (p value = < 0.0001). There was a statistically significant difference between post and 3-month errors (p value = 0.002) [20].
Ethical Considerations
Participants were given an Informed Consent Document Without Participant Signature prior to the start of the pre-test and education session [21]. It reviewed the purpose of mandatory education. It discussed the minimal risks and assured participants that results would remain secure and anonymous [22-24].
Results
The study assessed the effect of focused education on Vancomycin training on monitoring and compliance with prompting a decrease in Vancomycin discrepancies. All regularly employed full-time, part-time, and casually employed registered nurses on the two selected units were eligible to participate in the mandatory training. The total number of participants totaled (n=28). To complete the project, the participants were asked to complete a pre-test, post-test, and post three-month quiz.
Summary of Findings
Comparison of Pre-, Post- and Post Three-Month Quizzes
A Wilcoxon Signed Rank Test (non-parametric version of paired t-test) was performed to test if there was a difference between the numbers in (Table 1). There was a statistically significant difference (p-value = < 0.0001) between pre and post quiz scores incorrect items. There was also statistically significant difference (p-value = 0.002) between the 10-item incorrect quiz scores post- and three-month.
|
|
n |
Mean difference (post-pre) |
Standard deviation |
Median difference (post-pre) |
Wilcoxon Signed rank test statistic (S) |
p-value |
|
Post - Pre |
28 |
-2.04 |
1.32 |
-2.00 |
-162.5 |
<0.0001 |
|
3 Month - Post |
28 |
0.89 |
1.29 |
1.00 |
81.5 |
0.002 |
Table 1: Data Analysis of Pre and Post Mean Quiz Scores
(Table 2) displays a line graph with all three quizzes and their incorrect quiz answers. The average of each quiz is listed following each group. On this chart, average for pre-, post-, and three-month- respectively are three, one, and two.
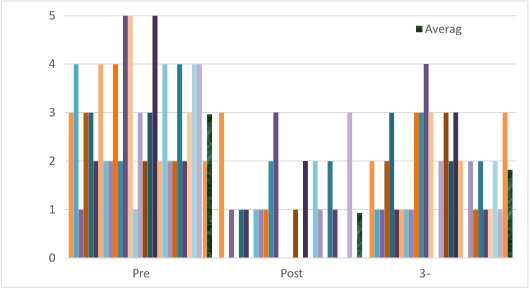 Table 2: Line Graph Total Number of Quiz Errors Pre-, Post- and Post-Three Month.
Table 2: Line Graph Total Number of Quiz Errors Pre-, Post- and Post-Three Month.
A Comparison of Both Patient Units: Medical and Progressive Care Unit (PCU)
A Chi-square test was performed to test if there was an association in discrepancy on the Medical Unit three months prior to education and three months post education noted in (Table 3). There is no statistically significant association.
|
Medical/Surgical |
Yes |
No |
Vancomycin Orders |
Chi-Square Test |
|
Prior to education April-June 2023 |
4 |
10 |
14 |
Χ2 = 0.04 p-value = 0.84 |
|
Post education July-September 2023 |
3 |
9 |
12 |
Table 3: Vancomycin Orders with Discrepancies (Medical/Surgical).
A Chi-square test was performed to test if there was an association in discrepancy in PCU Unit three months prior to education and three months post education noted in (Table 4).
There is a statistically significant association (p-value = 0.03).
|
Progressive Care Unit (PCU) |
Yes |
No |
Vancomycin Orders |
Chi-Square Test |
|
Prior to education April-June 2023 |
0 |
11 |
11 |
Χ2 = 4.89 p-value =0.03 |
|
Post education July-September 2023 |
4 |
7 |
11 |
Table 4: Vancomycin Orders with Discrepancies (Progressive Care Unit)
Observation Findings
The Vancomycin discrepancies on the Medical Unit prior and post education equal seven.
Reasons included for discrepancies were two retiming of dose, two mistimed lab levels, one physician order entry discrepancy, one generalized IV administration fault and one omitted dose by nursing. PCU equaled four discrepancies post education. Reasons included discrepancies, three MD order entry discrepancies and one omitted dose.
The Vancomycin Administration Data has been collected for three months thus far. For July 2023, discrepancies included two nursing-related events. One was listed as a discrepancy for timing of administration which was educated on in sessions, but the other was a medication discrepancy related to IV administration (not specific to Vancomycin). The second month of August 2023 showed two discrepancies related to physician ordering and not nursing administration. The third and final month of the EBQI project in September 2023 showed three total errors. Two errors were mistimed doses, and one was a physician order entry error. Many voiced acknowledgments of information during the sessions. At the beginning of October, a three-month post session quiz was completed by all registered nurses that took part in the sessions previously to validate the education regarding Vancomycin administration. The results reveal (refer to the chart) that learning was accomplished with the education sessions previously to validate the instruction.
Summary/Interpretation
Largely, this EBQI project was successful in educating the nurses regarding Vancomycin administration and monitoring compliance. This project identified at what level the discrepancies were occurring in the process. The nurses voiced understanding after the education sessions and acknowledged shortcomings with the policy. Lastly, the Director of Nursing and Pharmacy may adopt the education to all nursing staff following the pilot program pending results. This will be discussed with the Professional Practice Department about including this valuable education in nursing onboarding for all new hires and continued annually for all current employees. The benefit of education will support the evidence for Vancomycin compliance. Pharmacy will always be available as a resource for Vancomycin as questions arise during the transition and uninterrupted administrations. The continued attention to Vancomycin can benefit the organization, for example by decreasing repeat laboratory testing and inaccurately timed medication.
Limitations
Scheduling conflicts posed a concern for the education sessions. The Researcher rearranged sessions to accommodate schedules during the allotted project window. The original number of participants was n=31 that received the education session, completed the pre-and post- education quizzes. Three participants were removed from the project when they were unable to complete the post three-month quiz. Reasons for exclusion included medical leave and separation from employment. The final number of participants was n=28.
Recommendations for Future Studies
Education is needed for nursing to recognize the importance of Vancomycin administration and monitoring compliance on the patient units. The discrepancy rate for nursing has decreased after education. The inclusion of the “sidebar” on the eMAR for laboratory monitoring is a positive addition to Vancomycin compliance. This would benefit nursing to be introduced upon hire and have periodic staff education to ensure compliance with Vancomycin protocol can continue. In addition, unit and department “huddles” can convene for pharmacy and physician education to safeguard any identified misinformation regarding the order sets and medication policy.
Acknowledgments
I would like to personally thank everyone who has dedicated time and supported me with achieving my goal. It has been a long road.
Thank you to Dr. Kathleen Tennant, my mentor, for her continued direction and encouragement. I am extremely grateful for her honesty and candor.
This project could not have happened if it were not for the knowledge and commitment of Matt Clarkson, Lead Pharmacist. He was a solid piece in this education. He responded to every email and phone call anytime I needed him. I could not have done it without him.
My Community Expert, Anna Marie Pozycki guided me through the committees and requests as they arose. She also understands the need for future changes to improve outcomes. I value her support.
The Unit Managers and staff: Thank you for your cooperation with schedules and announcements. Nursing Staff was very welcoming to the education no matter what time I showed up on the unit.
My parents for supporting another educational journey. I always told them I was going to be a doctor.
Finally, my loving boys: My husband Jeff, son Jakob, and my four-legged assistant Dexter. I truly could not have done the last three years without you.
References
- Santalo O, Baig U, Poulakos M, Brown D (2016) Early Vancomycin Concentrations and the Applications of a Pharmacokinetic Extrapolation Method to Recognize Sub- Therapeutic Outcomes. Pharmacy 4: 37.
- Patel S, Preuss CV, Bernice F (2022) Vancomycin. StatPearls Publishing LLC.
- Peyko V, Friedman-Jakubovics M (2018) Novel approach to Vancomycin level monitoring: Impact of a multidisciplinary monitoring system on timing of Vancomycin levels. Am J Health Syst Pharm 75: 121-126.
- Shah S, Rouse GE, Mcmanus D, Tichy EM, Devaux L, et al. (2020) Optimizing the correct timing of Vancomycin level collection utilizing a Vancomycin medication administration record (MAR) level order. Int J Med Inform 143: 104249.
- Davis M (2022) Average Hospital Stay in US Costs 504 Hours of Work. Value Penguin.
- Siddiqui AH, Koirala J (2023) Methicillin-Resistant Staphylococcus aureus. StatPearls Publishing.
- Van Dort BA, Baysari MT, Carland JE, Stocker SL, Braithwaite HE, et al. (2020) Education to improve vancomycin use: the perspectives of educators and education recipients. Intern Med J 50: 565-572.
- Mishra V, Chouinard M, Keiser J, Wagner B, Yen M, et al. (2019) Automating Vancomycin Monitoring to Improve Patient Safety. Jt Comm J Qual Patient Saf 45: 757-762.
- Tung T, Delaurentis P, Yih Y (2022) Uncovering Discrepancies in IV Vancomycin Infusion Records between Pump Logs and EHR Documentation. Appl Clin Inform 13: 891-900.
- Abdel Jalil MH, Ηijazeen R, Abu-Mahfouz FK, Abu Hammour K, Matalqah MH, et al. (2023) Vancomycin prescribing and therapeutic drug monitoring: Challenges of real clinical practice. PloS one 18: e0285717.
- Melnyk BM, Tan A, Hsieh AP, Gallagher-Ford L (2021) Evidence-based practice culture and mentorship predict EBP implementation, nursing job satisfaction, and intent to stay: Support for the ARCC model. Worldviews Evid Based Nurs 18: 272-281.
- Scarano M, D'Arrigo S, De Letteriis S, Grasso S, Pittiruti M, et al. (2022) Risk of thrombophlebitis associated with continuous peripheral infusion of vancomycin: The effect of dilution. J Vasc Access 25: 107-112.
- Sault AD, Parent M, Simard C (2022) Methods of Therapeutic Drug Monitoring to Guide Vancomycin Dosing Regimens: Trough Concentration versus Ratio of Area Under the Curve to Minimum Inhibitory Concentration. Can J Hosp Pharm 75: 89-96.
- Zonozi R, Wu A, Shin JI, Secora A, Coresh J, et al. (2019) Elevated Vancomycin Trough Levels in a Tertiary Health System: Frequency, Risk Factors, and Prognosis. Mayo Clin Proc 94: 17-26.
- Krukas A, Franklin ES, Bonk C, Howe J, Dixit R, et al. (2020) Identifying Safety Hazards Associated with Intravenous Vancomycin Through the Analysis of Patient Safety Event Reports. Patient Safety 2: 31-47.
- gov (2023) ClinicalInfo HIV.gov. HIV.gov.
- Abulfathi AA, Chirehwa M, Rosenkranz B, Decloedt EH (2018) Evaluation of the Effectiveness of Dose Individualization to Achieve Therapeutic Vancomycin Concentrations. J Clin Pharmacol 58: 1134-1139.
- Becker ML, Baypinar F, Periboom M, Lilih S, Hoeven RTM, et al. (2021) The effect of medication related clinical decision support at the time of physician order entry. Int J Clin Pharm 43: 137-143.
- Chen TT, Liu MP, Sun HC (2022) Evaluation of Therapeutic Vancomycin Monitoring in Taiwan. Microbiol Spectr 10: e0156221.
- Chiwaula CH, Jere DL (2022) Experiences of nurse managers and practitioners on implementation of an evidence-based practice intervention. Health SA 27: 1597.
- Coleman LK, Wilson AS (2016) Impact of Nursing Education on the Proportion of Appropriately Drawn Vancomycin Trough Concentrations. J Pharm Pract 29: 472-474.
- Community Hospital Policy (2022) Vancomycin Protocol.
- Mahi-Birjand M, Ziaee M, Bijari B, Khalvati R, Abedini MR, et al. (2019) Evaluation of vancomycin use in university-affiliated hospitals in Southern Khorasan Province (East Iran) based on HICPAC guidelines. Drug Healthc Patient Saf 11: 29-35.
- McCain N, Ferguson T, Hultquist TB, Wahl C, Struwe L (2023) Influencing a Culture of Quality and Safety Through Huddles. J Nurs Care Qual 38: 26-32.
Appendix A
Appendix B
Appendix C
Appendix D
Vancomycin Pre-, Post-, and Post Three-Month Education Quiz
Unique Identifier
First letter of father’s first name (A–Z)
(Example: C for Charles)
First letter of mother’s first name (A–Z)
(Example: C for Carol) Birth month – “01–12” (Example: 07 for July) Birthday – “01–31”
(Example: 23 for 23rd of the month)
Total Identifier: CC0723 (Charles and Carol, July 23rd)
Please circle the correct answer.
- When should Vancomycin be administered if your patient is receiving hemodialysis?
- Before dialysis
- After dialysis
- Either one
- Patient is unable to receive this
- Where will Pharmacy communicate about Vancomycin dosing?
- In progress notes
- On MAR
- Over the phone
- In person
- Vancomycin STAT and/or Loading doses need to be administered within_______________________minutes of scheduled time?
- 15minutes
- 30 minutes
- 60minutes
- 90 minutes
- Do you hold the current dose of Vancomycin for current lab results of the trough level?
- Yes: The current dose is determined by the current level
- No: Since the level does not matter
- Yes: Only if the patient’s family says so
- No: The current level is used for monitoring and potential changes on upcoming doses
- If you lose IV access prior to dose of Vancomycin and are unable to obtain new access, what do you do?
- Retime the dose of medication
- Mark the medication as “not given ”
- Ask the physician for an oral dose of medication
- Call the pharmacy and tell them access was lost for the current dose
- A new patient arrives on the unit for administration of Vancomycin. What important data is relevant for proper dosing by pharmacy?
- Height (estimated).
- Vital signs
- Height and Weight (not estimated) and Serum Creatinine
- Temperature only.
Questions 7-10 are linked.
- The therapeutic window is small for Vancomycin to If a dose is due at 9am for a 2-hour infusion,
what is the latest you can administer the dose?
- 930am
- 10am
- 1030am
- 11am
- If ordered a trough level, when does it need to be obtained?
- 8am
- 830am
- 900am
- 930am
- If a peak level was ordered, when is the latest it must be obtained?
- 10am
- 1030am
- 11am
- 12pm
- Interventional Radiology calls for your patient at 845am to go for their They asked that no medications be administered during that time. You know the dose and trough are due- What do you do?
- Call the Pharmacy
- Reschedule the dose for dinner time
- Reschedule Interventional Radiology
- Chart the dose as “Not Given ”
Appendix E
Answers to all quizzes
Unique Identifier
First letter of father’s first name (A–Z)
(Example: C for Charles)
First letter of mother’s first name (A–Z)
(Example: C for Carol) Birth month – “01–12” (Example: 07 for July) Birthday – “01–31”
(Example: 23 for 23rd of the month)
Total Identifier: CC0723 (Charles and Carol, July 23rd)
- When should Vancomycin be administered if your patient is receiving hemodialysis?
- Before dialysis
- After dialysis (it will dialyze out of the body and not be effective)
- Either one
- Patient is unable to receive this medication
- Where will Pharmacy communicate about Vancomycin dosing?
- In progress notes (daily notes by pharmacy per protocol)
- On MAR
- Over the phone
- In person
- Vancomycin STAT and/or Loading doses need to be administered within_____________________minutes of scheduled time?
- 15minutes
- 30 minutes
- 60minutes
- 90 minutes
- Do you hold the current dose of Vancomycin for current lab results of the trough level?
- Yes: The current dose is determined by the current level.
- No: Since the level does not matter.
- Yes: Only if the patient’s family says so
- No: The current level is used for monitoring and potential changes on upcoming doses
- If you lose IV access prior to dose of Vancomycin and are unable to obtain new access, what do you do?
- Retime the dose of medication
- Mark the medication as “not given ”
- Ask the physician for an oral dose of medication
- Call the pharmacy and tell them access was lost for the current dose.
- A new patient arrives on the unit for administration of Vancomycin. What important data is relevant for proper dosing by pharmacy?
- Height (estimated)
- Vital signs
- Height and Weight (not estimated) and Serum Creatinine (This will determine if renal impairment is present prior to Serum creatinine is necessary to calculate the clearance)
- Temperature only
Questions 7-10 are linked.
- The therapeutic window is small for Vancomycin to If a dose is due at 9am for a 2-hour infusion,
what is the latest you can administer the dose?
- 930am
- 10am (60 minutes is the latest for Vancomycin dose accuracy)
- 1030am
- 11am
- If ordered a trough level, when does it need to be obtained?
- 8am
- 830am
- 900am
- 930am (30 minutes after the start of infusion)
- If a peak level was ordered, when is the latest it must be obtained?
- 10am
- 10: 30am
- 11am
- 12pm (At least 1hr after completion of the dose- up to 2 hours after dose)
- Interventional Radiology calls for your patient at 845am to go for their They asked that no medications be administered during that time. You know the dose and trough are due- What do you do?
- Call the Pharmacy (They will guide you per protocol how to proceed with dosing)
- Reschedule the dose for dinner time
- Reschedule Interventional Radiology
- Chart the dose as “Not Given”
Citation: O'Brien T (2024) The Peaks and Troughs of Vancomycin Compliance. J Pract Prof Nurs 8: 050
Copyright: © 2024 Tracy O'Brien, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.