Translation and Cross-Cultural Adaptation of the Revised Hearing Handicap Inventory Screening Tool into Asante-Twi
*Corresponding Author(s):
Sesi Collins AkoteySchool Of Rehabilitation Sciences, Faculty Of Health Sciences, University Of Ottawa, Ottawa, Canada
Email:scakotey@gmail.com / sakot030@uottawa.ca
Abstract
Objective: In line with the WHO recommendations for promoting global action for equitable access to ear and hearing care, this study aimed to translate and adapt the Revised Hearing Handicap Inventory Screening Tool (RHHI-S) into the Asante-Twi language.
Methods: Cross-cultural adaptation guidelines were followed to translate the RHHI-S from English into Asante-Twi. The steps included preparation, forward translation, synthesis/merge translation, back translation, expert committee review, field testing, and final translation. The final version of the Asante-Twi translation was administered to adults with varying hearing loss.
Results: The Asante-Twi version of the RHHI-S was judged to be culturally and linguistically appropriate with satisfactory semantic equivalence to the source version. The internal consistency of the instrument was high with a Cronbach’s alpha of 0.936, and a test-retest reliability of 0.946. The high internal consistency and ICC of the adapted Asante-Twi version of the RHHI-S corroborated the culture and linguistic appropriateness of the instrument for hearing loss screening.
Conclusion: The translated and adapted Asante-Twi version of the RHHI-S by the current study was culturally and linguistically appropriate. However, field validation to evaluate the complete psychometric properties of the Twi version is needed for the clinical use and hearing screening outcome measures for self-perceived hearing handicap in adults in Ghana.
Keywords
Asante-Twi; Cross-cultural adaptation; Hearing loss; Self-reported hearing measure; Translation
Introduction
Hearing is a critical sense and a key component of intrinsic human capacity. Any reduction in hearing can lead to severe consequences on interpersonal communication, quality of life, functional ability, economic independence, and general well-being [1,2]. Globally, 1.5 billion people experience hearing loss, of which 430 million would require hearing care [2]. The economic impact of unexamined hearing loss is approximately 950 billion international dollars annually [2]. Early identification via screening and appropriate management are vital in curbing the consequences of hearing loss. Hearing screening for at-risk individuals thus facilitates early identification, stimulates early management and intervention processes to reduce the impact of unidentified and untreated hearing loss. Hearing screening for early identification is therefore considered cost-effective [1], to mitigate the global burden of unexamined hearing loss.
Meanwhile, in sub- Saharan Africa, access to hearing care services appears to be extremely poor and inequitably distributed , compared to more affluent parts of the world [3]. Consequently, hearing screening at regular intervals for age-appropriate populations remains sub-optimal or virtually unavailable in sub-Saharan Africa despite the proven benefits [4]. The prevalence of hearing loss and the societal cost associated with unaddressed hearing loss in adults living in sub-Saharan Africa, specifically in Ghana, highlights the need to develop effective hearing healthcare services.
Different hearing screening techniques have been proposed to improve hearing health care over the last 50 years. For example, hearing screenings using smartphones promise to bring hearing health care to underserved communities [5]. Self-reported measures of hearing difficulties or hearing handicap have also been proven as a valuable instrument to screen for hearing loss [6]. Self-reported measures are relatively low-cost and time efficient in their administration. Furthermore, self-reported hearing disability is positively linked with help-seeking among adults [7].
Self-reported measures are relatively new in hearing screening, and there are relatively few validated instruments. The Revised Hearing Handicap Inventory and Screening tool (RHHI-S; Cassarly et al. [8]) is an example of a validated self-reported instrument. This ten-item screening questionnaire was created with items that are common to both the Hearing Handicap Inventory for the Elderly (HHIE; Ventry & Weinstein [9]) and the Hearing Handicap Inventory for Adults (HHIA; Newman et al. [10]). Both the HHIE and HHIA are well-established questionnaires with validated psychometric properties used to evaluate the self-perceived effect of hearing loss [9-13]. Compared with the HHIE and HHIA, the RHHI-S has also been validated and can be used for hearing screening of adults of all ages [8].
Each item of the RHHI-S can be answered with “No," “Sometimes," or “Yes," which corresponds to a specific score, i.e., 0 for "No," 2 for “Sometimes,” and 4 for "Yes." The total score can then be computed and compared to a scale of hearing handicap, ranging from 0 (“no handicap”) to 40 (“maximum handicap”) or used for identifying people at risk of hearing loss. According to the authors, a score between 0-8 suggests “no hearing handicap” or a 13% probability of hearing impairment, whereas a score between 10-24 points implies a 50% probability of hearing impairment. Finally, a score between 26-40 points indicates an 84% probability of hearing impairment [8]. A cutoff of ≥6 is recommended for screening purposes and to detect hearing loss [8].
Hearing screening questionnaires are available for adults in different languages [14,15], but none is available in any Ghanaian language. There are close to 80 languages spoken in Ghana [16]. Asante-Twi is one of the four mutually intelligible dialects spoken by the Akans. It is among the nine languages being sponsored by the government, meaning it is taught and learnt in many Ghanaian schools [17,18]. Akan represent the largest ethnic group in Ghana [16,19]. For instance, 81.7% of the Central region populace, and 78.2% and 74.2% of the populace in the Western and Ashanti regions respectively of Ghana are Akans [19].
The present study aimed to translate and adapt the RHHI-S into Asante-Twi. Since most of the available self-report hearing questionnaires were developed using a well-established framework, translation and cross-cultural adaptation of existing instruments have clear advantages over creating new ones [20,21]. Hall et al. [20], have synthesized existing recommendations for cross-cultural adaptation in promoting good practice in the Audiology community. Their guideline and recommendations were used for this study.
Materials And Methods
The 7-step translation process, as recommended by Hall et al. [20], was followed (Figure 1) for the translation and adaptation of the original version of the RHHI-S into the Asante-Twi language. It involved cultural and language considerations to maintain the concepts and meaning from the original version while ensuring cultural equivalence and appropriateness.
A total of 87 participants were recruited for the pre-testing and field evaluation of the adapted instrument. In the pre-testing, 32 participants took part in the cognitive evaluation of the adapted Asante-Twi version for its cultural equivalence and linguistic appropriateness. While 55 participants participated in the field testing to investigate the basic psychometric properties of the instrument.
Thirty-two participants for the pre-testing were recruited via social media platforms (WhatsApp) via invitation to participate in the study. Information about the study was shared on WhatsApp group platforms for university students and clients of Center Hearing and Services, Winneba. Interested participants contacted the researcher privately through their social media contact and were later sent the instrument. According to Hall et al. [20], a sample size of at least 20 participants should be used for the pre-testing where there are regional variations and to ensure the original instructions, items and scoring materials are clearly expressed. In the field testing, participants who attended audio logical services at the Centre for Hearing and Speech Service (CHSS), Winneba, Ghana were recruited after an explanation of the instrument has been presented to them and they consented to participate. A sample size of 50 was used as recommended by Hall et al. [20], to evaluate the internal consistency and test-retest reliability of the adapted Asante-Twi version of the RHHI-S. Participants of the present study were aged between 18 and 73 years; were all living in Ghana and able to read and speak English and Asante-Twi. The seven steps of the translation and cultural adaptation of RHHI-S into Asante-Twi are described in the following paragraphs and illustrated in figure 1.
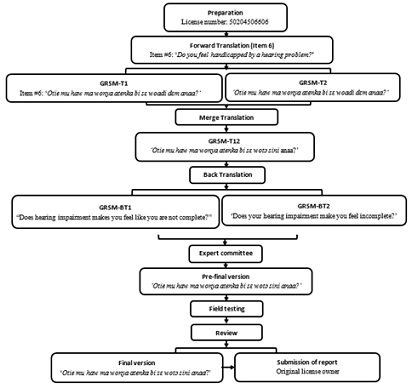
Figure 1. Stages of the translation and cross-cultural adaptation of the RHHI-S into the Asante-Twi language. Item #6 of the questionnaire was used to illustrate the different stages of the process.
Note: Steps in cross-cultural translation and adaptation process. Adapted from “A good practice guide for translating and adapting hearing-related questionnaires for different languages and cultures,” by [20].
Preparation: A search in the literature was conducted to ensure the Asante-Twi version of the RHHI-S did not already exist. Findings confirmed that no versions of the RHHI-S existed in any Ghanaian language, including Asante-Twi. Following this confirmation, written permission, and a license to translate and adapt the instrument was granted by the copyright holders.
Forward Translation: Two bilingual language experts, whose mother tongue is Asante-Twi and who are fluent in English, independently translated the instrument from its original version to Assante-Twi. These language experts are professionals who hold at least of Bachelor of Arts degree in Twi from the School of Languages, University of Education, Winneba, Ghana. The first author briefed the language experts about the instrument and the translation process. These Asante-Twi versions of RHHI-S were code-named GSRM-T1 and GSRM-T2.
Merge Translation: Another independent and unbiased bilingual language expert, fluent in Asante-Twi and English, merged the two forward translations (GSRM-T1 and GSRM T2) into a single document. Differences between the two initial translations were discussed and resolved by consensus among the three translators. The merged translation was called the GSRM-T12.
Back Translation: Two other independent language experts translated the merged translation (GSRM-T12) into English. The back-translation was to validate the accuracy of the translation and ensure it reflected the item content as the source instrument. Without prior knowledge of the source instrument, the language experts produced two separate English translations of the merged translation, GSRM-BT1 and GSRM-BT2.
Expert Committee Review: A panel of experts comprising two audiologists, a language expert from the School of Languages, University of Education, Winneba; an educator of persons who are deaf and hard of hearing, and the forward and back translators, discussed the backward translation and produced a pre-final version of the instrument for field testing in Ghana. The discussion was conducted by teleconference and aimed to achieve the instrument's semantic, idiomatic, experimental, and conceptual equivalence and complete the questionnaire's Pre-final version. All the members of the committee were living in Ghana and fluent in both Asante-Twi and English. The first author was in contact with the committee in the waiting room throughout their meeting to provide any clarifications that may be needed concerning the concepts being measured by the questionnaire.
Field Testing: This was conducted in two stages-cognitive debriefing and pilot-testing of the instrument
- Cognitive Debriefing: In line with Hall et al. [20], guideline, a pre-testing of the Asante-Twi translation was conducted with participants who were fluent in English and Asante-Twi. Interviews were conducted with each participant. The aim was to ensure the Asante-Twi translation’s instructions, the items/questions, and the scoring were straightforward. The understanding level of the items and semantic equivalence, the cultural relevance and the acceptability of the instrument were also assessed. Each participant was invited to complete the Asante-Twi translation of the instrument online, followed by a semi-structured interview. The first author conducted all the interviews, which aimed to evaluate the ease of understanding the instrument’s items and identify any ambiguity. Participants were also asked to report any difficult questions to understand and to make any suggestions to improve clarity. A simple seven-response Likert scale was used to record participants’ responses, using the following categories: “Strongly disagree, Disagree, Somewhat disagree, Neutral, Somewhat agree, Agree, and strongly agree.” Participants’ opinions, responses and suggestions were analyzed to consolidate the correctness of the Asante-Twi translation and, where necessary, to incorporate changes for the final version of the adapted and the translated version (Asante-Twi).
- Pilot Testing: The instrument's pre-final version was administered to participants of the target population who attended audio logical services at the CHSS. Participants completed the instrument twice with a two-week interval between the first and second completion of the instrument. The internal consistency and test-retest reliability of the adapted instrument were examined. The internal consistency examined the degree of the interrelationship among the items on the instrument and how reliably the items can measure the same construct. The Cronbach's alpha coefficient was used to evaluate the internal consistency of the adapted instrument to measure self-perceived handicap. An interval consistency defined by Cronbach's alpha coefficient of 0.7 is considered the minimally acceptable level for the interrelatedness of the test items. Test-retest reliability measures the reliability/consistency obtained by administrating the same test twice on the same sample at a different point in time. The Intraclass Correlation Coefficient (ICC) was used to assess the agreement between the total scores in the two administrations of the instrument-test-retest reliability.
Results
A pre-testing with 55 participants who were representatives of the target population was conducted. There were twenty-seven (27) females - representing 49.1%, and twenty-eight (28) males representing 50.9%, with a mean age of 42 years (Table 1).
|
Characteristic |
Mean |
SD (%) |
N |
% |
|
Age (Years) |
42 |
16.42 |
|
|
|
Male Gender |
|
|
28 |
50.9 |
|
Female Gender |
|
|
27 |
49.1 |
|
Total |
|
|
55 |
100 |
Table 1: Sample demographics for field testing (n=55).
Cognitive Debriefing: All participants (100%) strongly agreed that the items were clear and understandable. Participants further disagreed or strongly disagreed (100%) that words or phrases in the instrument's items were difficult. Again, participants unanimously (100%) disagreed with making any changes to any questions. Participants scored the clarity of the items on a scale of one (1) to seven (7) on the Likert scale, where one (1) represented strongly disagree and seven (7) strongly agree. Scores for the clarity of the items in the adapted instrument and instructions ranged from 6 to 7 out of 7. A score above 4 indicates that the items are clear and do not require revision [22,23]. As a result, there were no changes made to the pre-final version of the instrument regarding words or phrases as participants suggested clarity and understanding of the individual items. All the items and wording were culturally relevant, intelligible, and non-offensive.
Results from the pilot testing showed that the overall internal consistency of the adapted and translated version for the 10 items was 0. 936. The test-retest reliability of the instrument was assessed using the Intraclass Correlation Coefficient (ICC), yielding a substantial agreement of 0.946 with a 95% confidence interval between 0.921 and 0.965 (Table 2).
|
|
ICC |
95% Confidence Interval |
F Test with True Value 0 |
||||
|
Lower Bound |
Upper Bound |
Value |
df1 |
df2 |
Sig |
||
|
Average Measures |
0.946c |
0.921 |
0.965 |
18.379 |
54 |
486 |
0.000 |
Table 2: Test-retest reliability of the Asante-Twi version.
Note: ICC absolute agreement.
Discussion
The study aimed to translate and adapt the RHHI-S into Asante-Twi. Asante-Twi is considered the most widely spoken dialect in Ghana [19]. The guideline and recommendations from Hall et al. [20], were used to achieve linguistic and cultural equivalence between the source instrument (RHHI-S) and the translated and adapted version in Asante-Twi. Interviews conducted with participants from the Ghanaian population suggested that the cultural equivalence and content validity of the Asante-Twi version of the RHHI-S was satisfactory. The words and sentences of this adapted version of the instrument were judged culturally appropriate, and non-offensive with satisfactory semantic equivalence to the source version.
During the pilot testing of the pre-final version of the Asante-Twi RHHI-S, participants did not show any difficulty completing the items. This could be attributed to the successful, cultural equivalence and linguistic appropriateness of the adapted and translated Asante-Twi version of the RHHI-S translation.
The internal consistency of the Asante-Twi version of the RHHI-S was evaluated by estimating Cronbach’s alpha value. Results for the investigation showed a high internal consistency of the adapted instrument, thus, a Cronbach's alpha coefficient of α=0.936. This is indicative of a strong internal consistency of the test items. To a larger extent, the scores obtained from these 10 items are consistent and dependable, making the adapted and translated version a reliable instrument for assessing the intended construct. This finding is consistent with the findings of Newman et al. [24], indicating the instrument’s ability to measure the construct of self-perceived handicap.
Investigating the test-retest reliability of the Asante-Twi version using the intraclass correlation coefficient showed high test-retest reliability of the test items with an ICC score of 0.946 for all the items. This finding indicates a high level of reliability in the test-retest measurements of the Asante-Twi Version, as supported by the significant F test and a narrow confidence interval around the ICC. These findings are similar to that of the source instrument [8], showing stability and high reliability in the test-retest ability of the instrument. Newman et al. [24], reported test-retest reliability to range from 0.93 to 0.97.
Notwithstanding these findings, further investigations of the instrument the psychometric properties (predictive validity, and construct validity), sensitivity, specificity, and the cut-off point of the Asante-Twi version of the RHHI-S need to be assessed before this hearing screening is used clinically.
Strengths and Limitations
A strength of the current study was the adherence to the guideline provided for the cross-cultural translation and adaptation. As described in Hall et al. [20], guideline, each step was followed, resulting in the cultural relevance and satisfactory semantic equivalence of the translated and adapted versions. The study also used participants from the target population [25-27].
A limitation of the present study is that the sample of participants did not necessarily represent native Asante-Twi speaking Ghanaian population with specific reference to location. Participants for the current study were recruited from one geographical location - Winneba. There is a need for a more representative sample of Asante-Twi populace. This could be considered and implemented during the validation of the adapted questionnaire.
Conclusion
The development of validated and culturally adapted hearing instrument tools is in line with WHO’s recommendations of promoting actions for equitable access to ear and hearing care across the world. The present study's objective was to translate and adapt the RHHI-S into Asante-Twi, one of Ghana's most spoken languages. The translated and adapted Asante-Twi version of the RHHI-S by the current study was culturally and linguistically appropriate. However, the psychometric properties (predictive validity, construct validity, and concurrent validity) of the Asante-Twi version of the RHHI-S need to be assessed before it is used as a hearing screening tool.
Declaration of Interest
The authors declared no potential conflicts of interest concerning the translation and adaptation, authorship, and/or publication of this article. The authors are responsible for the content and writing of the article.
Acknowledgment
The authors are thankful to members of the expert committee; Nicholas Obeng Agyekum, Cyril Mawuli Honu-Mensah, George Kweku Danful, and Emmanuella Ampabeng; and the translators; Derrick Oppong, Seth Amoah, Samuel Boakye, Stephen Asante and Prince Osei Mensah, for their role in the translation process. We are grateful to Yaw Nyadu Offei (Ph.D.) and Mawuli Tay for their helpful discussions regarding the cultural relevance of the paper and the analysis of the data sets. The authors are also thankful to all participants.
References
- World Health Organization (2017) Global costs of unaddressed hearing loss and cost-effectiveness of interventions. World Health Organization, Geneva, Switzerland.
- World Health Organization (2021) World report on hearing. World Health Organization, Geneva, Switzerland.
- Mulwafu W, Kuper H, Ensink RJH (2016) Prevalence and causes of hearing impairment in Africa. Trop Med Int Health 21: 158-165.
- Mulwafu W, Ensink R, Kuper H, Fagan J (2017) Survey of ENT services in sub-Saharan Africa: Little progress between 2009 and 2015. Glob Health Action 10: 1289736.
- Hussein SY, Swanepoel DW, de Jager, LB, Myburgh HC, Eikelboom RH, et al. (2016) Smartphone hearing screening in mHealth assisted community-based primary care. J Telemed Telecare 22: 405-412.
- Smits C, Kramer SE, Houtgast T (2006) Speech reception thresholds in noise and self-reported hearing disability in a general adult population. Ear Hear 27: 538-549.
- Knudsen LV, Öberg M, Nielsen C, Naylor G, Kramer SE (2010) Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: A review of the literature. Trends Amplif 14: 127-154.
- Cassarly C, Matthews LJ, Simpson AN, Dubno JR (2020) The revised hearing handicap inventory and screening tool based on psychometric reevaluation of the hearing handicap inventories for the elderly and adults. Ear Hear 41 95-105.
- Ventry IM, Weinstein BE (1982) The hearing handicap inventory for the elderly: A new tool. Ear Hear 3: 128-134.
- Newman CW, Weinstein BE, Jacobson GP, Hug GA (1990) The hearing handicap inventory for adults: Psychometric adequacy and audiometric correlates. Ear Hear 11: 430-433.
- Chisolm TH, Johnson CE, Danhauer JL, Portz LJP, Abrams HB, et al. (2007) A systematic review of health-related quality of life and hearing aids?: Final report of the American academy of audiology task force on the health-related quality of life benefits of amplification in adults. American Academy of Audiology 183: 151-183.
- Hospers JMB, Smits N, Smits C, Stam M, Terwee CB, et al. (2016) Reevaluation of the Amsterdam inventory for auditory disability and handicap using item response theory. Journal of Speech, Language, and Hearing Research 59: 373-383.
- Lazzarotto S, Baumstarck K, Auquier P (2016) Age-related hearing impairment and impact on quality of life: A review of available questionnaires. Ann Otolaryngol Rhinol 3: 1107.
- Laohasiriwong S, Kasemsiri P, Thanavirathananich P, Yimtae K (2018) Validity and Test-Retest Reliability of Hearing Handicap Inventory for the Elderly Thai Version (HHIE-Thai). Annals of Otolaryngology and Rhinology 5: 1204.
- Thammaiah S, Manchaiah V, Easwar V, Krishna R (2016) Translation and adaptation of five English language self-report health measures to South Indian Kannada language. Audiology Research 6: 1-3.
- Appiah SO, Ardila A (2020) The question of school language in multilingual societies: the example of Ghana. RUDN Journal of Psychology and Pedagogics 17: 263-272.
- Agbozo GE (2015) Language choice in Ghanaian classrooms: Linguistic realities and perceptions. Norwegian University of Science and Technology.
- Owu-Ewie C (2003) The language policy of education in Ghana: A critical look at the English-only language policy of education. Project Management Journal 33: 171-175.
- Ghana Statistical Service (2013) 2010 Population & Housing Census National Analytical Report. Ghana Statistical Service 1-91.
- Hall DA, Domingo SZ, Hamdache LZ, Manchaiah V, Thammaiah S, et al. (2018) A good practice guide for translating and adapting hearing-related questionnaires for different languages and cultures. Int J Audiol 57: 161-175.
- Wild D, Eremenco S, Mear I, Martin M, Houchin C, et al. (2009) Multinational trials - Recommendations on the translations required, approaches to using the same language in different countries , and the approaches to support pooling the data: The ISPOR patient-reported outcomes translation and linguistic validation good research practices task force report. Value Health 12: 430-440.
- Tremblay D, Poder TG, Vasiliadis HM, Touati N, Fortin B, et al. (2020) Translation and cultural adaptation of the patient self-administered financial effects (P-safe) questionnaire to assess the financial burden of cancer in French-speaking patients. Healthcare 8.
- Vallerand RJ (1989) Towards a methodology for transcultural validation of psychological questionnaires: Implications for research in the French language. Psychol Can 30: 662-689.
- Newman CW, Weinstein BE, Jacobson GP, Hug GA (1991) Test-retest reliability of the hearing handicap inventory for adults. Ear and Hearing 12: 355-357.
- Bland J, Altman D (1997) Statistics notes: Cronbach’s alpha. British Medical Journal 314: 572.
- Chou R, Dana T, Bougatsos C, Fleming C, Beil T (2011) Screening adults aged 50 years or older for hearing loss: A review of the evidence for the U.S. preventive services task force. Annals of Internal Medicine 154: 347-355.
- Offei YN (2017) Audiology in Ghana.
Citation: Akotey SC, Lagacé J, Sauvé-Schenk K, Giguère C (2023) Translation and Cross-Cultural Adaptation of the Revised Hearing Handicap Inventory Screening Tool into Asante-Twi. J Otolaryng Head Neck Surg 10: 087.
Copyright: © 2024 Sesi Collins Akotey, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.