Treatment of Juvenile X-Linked Retinoschisis with Topical Ketorolac and Dorzolamide
Abstract
A 27-year-old healthy white male presented with slow onset decreased vision in both eyes for many years. He denied any past medical or past ocular history. Best-corrected visual acuity was 20/80 in both eyes. Cystoid macular schisis due to juvenile X-linked retinoschisis was diagnosed in both eyes based on ophthalmic exam, SD-OCT, and fluorescein angiography. Treatment was initiated with topical ketorolac 0.5%, a Non-Steroidal Anti-Inflammatory Drug (NSAID), four times a day in both eyes. Oral acetazolamide, a Carbonic Anhydrase Inhibitor (CAI), was later added. Acetazolamide was replaced with topical dorzolamide 2% twice a day in both eyes due to the patient’s reluctance to use systemic CAIs. Over several months, the treatment regimen resulted in improved visual acuity to 20/30 in both eyes and decreased macular thickness.
Keywords
INTRODUCTION
Juvenile X-linked retinoschisis belongs to a group of the vitreoretinal dystrophies [1]. It is characterized by bilateral maculopathy and peripheral retinoschisis in half of the patients [2]. The basic defect is in the retinoschisin protein, which is expressed in photoreceptors of the inner and outer layers of the retina. This defect leads to splitting of the retinal nerve fiber layer, plexiform, and nuclear layers from the rest of the sensory retina [3]. The inheritance is X-linked as the name suggests, and the gene implicated has been identified as the RS1 gene [4]. The prevalence is estimated to be 1 in 15,000 to 1 in 30,000 [1]. Affected males usually present in the first decade of life due to decreased visual acuity. Long-term visual outcomes can be poor due to the limited number of known successful treatments. We present an alternative treatment, in which visual acuity improved with the use of topical ketorolac and dorzolamide.
CASE PRESENTATION
A 27-year-old otherwise healthy male was referred for slow onset of decreased vision in both eyes for many years. His past medical history and his past ocular history were negative. He reported no relevant family history. His initial best-corrected visual acuity was 20/80 in both eyes. His anterior segment exam was unremarkable. Posterior segment examination revealed cystoid macular edema in both eyes. Peripheral retinal examination showed lattice degeneration in both eyes and a vitreoretinal tuft in his left eye. Red-free fundus photos showed foveal schisis in both eyes (Figure 1). Copernicus Spectral Domain Optical Coherence Tomography (SD-OCT) confirmed the suspicion of cystoids macular schisis in both eyes (Figure 2). Fluorescein angiography showed no significant late leakage in the macula (Figure 3). The differential diagnosis for Cystoid Macular Edema (CME) without leakage could be Goldman-Favre syndrome, juvenile X-linked retinoschisis, retinitis pigmentosa, medication induced CME (i.e., nicotinic acid and prostaglandins), and autosomal dominant CME. Our initial diagnosis was cystoid macular schisis caused by juvenile X-linked retinoschisis.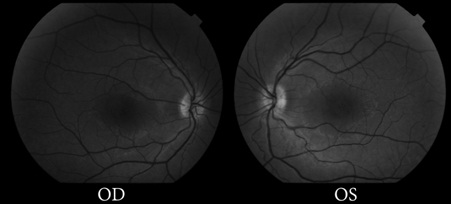
Figure 1: Red-free fundus photographs showing foveal schisis in both eyes.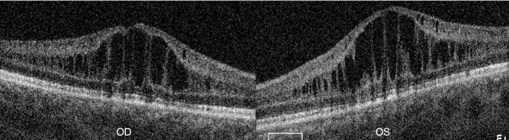
Figure 2: SD-OCT on presentation shows cystoid macular changes consistent with XLRS in both eyes. Split retinal layers are connected by vertical palisades, giving a cyst-like appearance.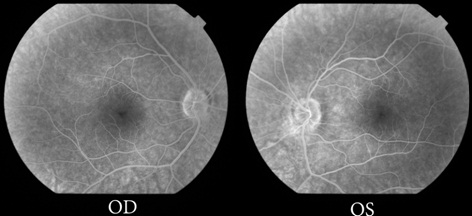
Figure 3: Late frames of fluorescein angiography showed no significant leakage in either eye.
The patient was started on ketorolac 0.5% topical drops four times a day in both eyes for the maculopathy. He returned after 8 weeks, at which this time his vision improved to 20/30 in both eyes, with improved macular cysts (Figure 4). At this time oral acetazolamide 250 mg twice a day was added to try to maximize therapeutic effect. One month later, his visual acuity remained at 20/30 in both eyes, with largely unchanged cysts in both eyes (Figure 5). Due to the patient’s reluctance to take oral medications, he was instead treated with topical dorzolamide 2% twice a day in both eyes. Two months later on chronic therapy with ketorolac four times a day and dorzolamide twice a day in both eyes, his vision remained stable at 20/30 in both eyes. On SD-OCT at this time, the macula was flat with a few tiny cysts in the right eye and the left eye had only a few cysts remaining (Figure 6). Electroretinogram was inconclusive, and genetic testing was not performed.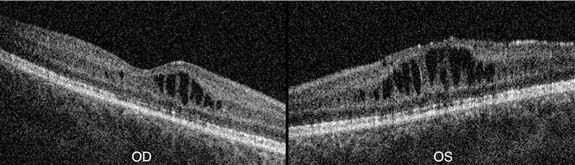
Figure 4: After 8 weeks of treatment with topical ketorolac four times a day in both eyes, visual acuity improved, with improvement of the macular cysts on SD-OCT in both eyes. 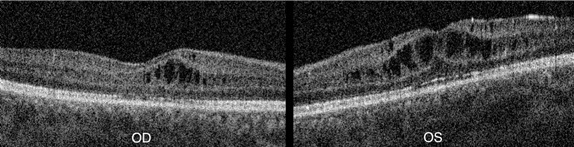
Figure 5: After 1 month of treatment with oral acetazolamide, to which the patient admitted poor compliance, SD-OCT shows minimal change of the macular cysts in both eyes. 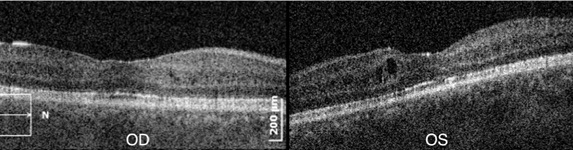
Figure 6: On chronic therapy with topical dorzolamide and ketorolac, vision stabilized at 20/30 OU. On SD-OCT, there were a few tiny remaining cysts in the right eye and few cysts in the left eye.
DISCUSSION
The cause of decreased visual acuity in patients with juvenile X-linked retinoschisis is foveal schisis, which appears as cysts on SD-OCT. When topical dorzolamide is used, the fovea may be able to return to normal morphology and in some cases, visual acuity may improve substantially. Carbonic anhydrase inhibitors, in the oral or topical form, may increase the retinal pigment epithelial pumping function and also increase intraretinal fluid absorption [5-7]. An extracellular membrane-bound carbonic anhydrase in the brain and retina is the target of dorzolamide. [8]. Carbonic anhydrase inhibitors have been shown to be helpful in the treatment of macular cystoid changes associated with X-linked retinoschisis. Several authors have also reported a clinically significant improvement in visual acuity [9-12].
Although there have been many studies examining the effects dorzolamide on macular edema, there are no reports of using a topical Non-Steroidal Anti-Inflammatory (NSAID) for X-linked retinoschisis-related maculopathy. Ketorolac is a topical NSAID used for a wide variety of pathologies including ocular inflammation and pseudophakic cystoid macular edema [13-15]. In this patient with juvenile X-linked retinoschisis, we elected to initiate therapy with a topical NSAID due to the findings by Joshi et al., that intraschisis cavity fluid is composed of tenascin-C (an extracellular matrix protein involved in wound healing) and cystatin C (a ubiquitous cysteine protease inhibitor implicated in inflammation) [16]. In our case, there was marked improvement in visual acuity and in macular cyst size following monotherapy with topical ketorolac. The addition of dorzolamide possibly resulted in a synergistic effect, with near complete resolution of the macular cysts in one eye, and complete normalization of the macular contour in the other eye after 4 months of treatment. Further studies would be needed to compare topical NSAID alone, topical CAI alone, and combination therapy of the two.
The results of our case study suggest that the use of the topical form of CAI, in combination with topical NSAID, should be considered and studied further for a possible treatment of juvenile X-linked retinoschisis related maculopathy.
REFERENCES
- De La Chapelle A, Alitalo T, Forsius H (1994) X-linked juvenile retinoschisis.In: Wright AF, Jay B (eds.). Molecular Genetics of Inherited Eye Disorders, Harwood Academic Publishers, Newark, New Jersey, USA Pg: 339-357.
- Kellner U, Brümmer S, Foerster MH, Wessing A (1990) X-linked congenital retinoschisis. Graefes Arch Clin Exp Ophthalmol 228: 432-437.
- Salvatore S, Fishman GA, Genead MA (2013) Treatment of cystic macular lesions in hereditary retinal dystrophies. Surv Ophthalmol 58: 560-584.
- Sauer CG, Gehrig A, Warneke-Wittstock R, Marquardt A, Ewing CC, et al. (1997) Positional cloning of the gene associated with X-linked juvenile retinoschisis. Nat Genet 17: 164-170.
- Genead MA, Fishman GA, McAnany JJ (2010) Efficacy of topical dorzolamide for treatment of cystic macular lesions in a patient with enhanced S-cone syndrome. Doc Ophthalmol 121: 231-240.
- Hajali M, Fishman GA (2009) Dorzolamide use in the management of macular cysts in a patient with enhanced S-cone syndrome. Retin Cases Brief Rep 3: 121-124.
- Iannaccone A, Fung KH, Eyestone ME, Stone EM (2009) Treatment of adult-onset acute macular retinoschisis in enhanced s-cone syndrome with oral acetazolamide. Am J Ophthalmol 147: 307-312.
- Nagelhus EA, Mathiisen TM, Bateman AC, Haug FM, Ottersen OP, et al. (2005) Carbonic anhydrase XIV is enriched in specific membrane domains of retinal pigment epithelium, Muller cells, and astrocytes. Proc Natl Acad Sci USA 102: 8030-8035.
- Khandhadia S, Trump D, Menon G, Lotery AJ (2011) X-linked retinoschisis maculopathy treated with topical dorzolamide, and relationship to genotype. Eye (Lond) 25: 922-928.
- Bastos AL, Freitas Bde P, Villas Boas O, Ramiro AC (2008) Use of topical dorzolamide for patients with X-linked juvenile retinoschisis: case report. Arq Bras Oftalmol 71: 286-290.
- Apushkin MA, Fishman GA (2006) Use of dorzolamide for patients with X-linked retinoschisis. Retina 26: 741-745.
- Genead MA, Fishman GA, Walia S (2010) Efficacy of sustained topical dorzolamide therapy for cystic macular lesions in patients with X-linked retinoschisis. Arch Ophthalmol 128: 190-197.
- Heier JS, Topping TM, Baumann W, Dirks MS, Chern S (2000) Ketorolac versus prednisolone versus combination therapy in the treatment of acute pseudophakic cystoid macular edema. Ophthalmology 107: 2034-2038.
- Weisz JM, Bressler NM, Bressler SB, Schachat AP (1999) Ketorolac treatment of pseudophakic cystoid macular edema identified more than 24 months after cataract extraction. Ophthalmology 106: 1656-1659.
- Sivaprasad S, Bunce C, Crosby-Nwaobi R (2012) Non-steroidal anti-inflammatory agents for treating cystoid macular oedema following cataract surgery. Cochrane Database Syst Rev 2: CD004239.
- Joshi MM, Drenser K, Hartzer M, Dailey W, Capone A, et al. (2006) Intraschisis cavity fluid composition in congenital X-linked retinoschisis. Retina 26: 57-60.
Citation: Andersen A, Schadlu A (2015) Treatment of Juvenile X-Linked Retinoschisis with Topical Ketorolac and Dorzolamide. J Clin Stud Med Case Rep 2: 010.
Copyright: © 2015 Austin Andersen, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.